i bc27f85be50b71b1 (173 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown

GASrROINTISTINAl SYSTEM
555
46. Gavaghan M. Anatomy and physiology of the esophagus. AORN J
I 999;69(2):372( I ).
47. Knudsen JF, Friedman B, Chcn M, Goldwasser jE. Ischemic colitis and
.umatriptan use. Arch Intern Med 1998; 158( 17): 1946-1948.
48. Voelker R. Bacteria and irritable bowel. JAMA 200 I ;285(4):401.
49. Jailwala J, Imperiale TF, Kroenke K. Pharmacologic trcatmem of the
irritable bowel s}'ndrome: a systematic review of randomized, controlled
trials. Ann Intern Med 2000;133(2):136.
50. Bayless TM, Hendrix TR. Malabsorption. In JD Swbo, DB Hellmann,
PW Ladenson, et al. leds), The Principles and Practice of Medicine (23rd
ed). Stamford Cf: Appleton & Lange, 1996;485-495.
51. Bonci L, Fasano A, Goff JS, et al. Is malabsorption causing your
patient's GI symptoms? Paticnt Care 1998;32(6):93.
52. Krige JEJ, Beckingham IJ. ABC of diseases of liver, pancreas, and biliary
system: porral hypertension-2. Ascites, encephalopathy, and other conditions. BMJ 2001 ;322(7283):416-18.
53. Navez B. Laparoscopic managemem of acute peritonitis. Br J Surg
1998;85:32-36; Abstract in JAMA 1998;279( 12):896U.
54. Bayless TM, Harris ML. Inflammatory Bowel Disease. In JD Stobo, DB
Hellmann, PW Ladenson, ct 31. leds), The Principles and Practice of
Medicine (23rd cd). Stamford Cf: Appleton & Lange, 1996;496-503.
55. Blumberg RS, Strober W. Prospects for research in inflammatory bowel
disease. JAMA 200 I ;285(5):643.
56. Schreiber . afety and efficacy of recombinant human imerleukin lOin
chronic active Crohn's disease. JAMA 200 I ;285( I I ): 1421.
57. Galper C, Cerda J, Hanauer SB, et al. Inflammatory bowel disease:
guidelines for management. Patient Care 1998;32(5):81.
58. Colorectal Pol)'ps: Latest Guidelines for Detection and Follow-up. Consultant 2001 ;41 (3):364.
59. Cramer DA. Hepatitis. In K Boyden, D Olendorf (cds), Gale Encyclopedia of Medicine. Farmington Hills, MI: Gale Group, 1999;1421-1422, 1425-1433.
60. Mitchell Me. Acute Hepatitis. In JD Stobo, DB Hellmann, PW Ladenson, et al. (eds), The Principles and Practice of Medicine (23rd ed).
Stamford Cf: Appleton & Lange, 1996;516-525.
61. Goodman Cc. The Hepatic, Pancrearic, and Biliary Systems. In CC
Goodman, WG Boisonnaulr (cds), Pathology: Implicarions for the Physical Therapist. Philadelphia: Saunders, 1998;496-531.
62. Beckingham IJ. ABC of diseases of liver, pancreas, and biliary system.
Gallstone disease. BMJ 2001 ;322(7278):9·1.
63. Aronson BS. Update on acute pancreatitis. Medsurg Nurs 1999;8( I ):9-
16.
64. Chronic Pancreatitis. In GL Eastwood, C Avunduk (cds), Manual of
Gastroenrerology (2nd ed). Boston: Little, Brown, 1994;309.
65. Pancreatic Cancer. In GL Easrwood, C Avunduk (cds), Manual of Gas
(roenteroiog), (2nd cd). Boston: Little, Brown, 1994;313.
66. Pedersen AG. Randomized clinical £rial of laparoscopic versus open
appendicectomy. JAMA 2001 ;285( 15):1942.

556 AClITE CARE HANDBOOK FOR PHYSICAL THERAI'ISTS
67. McMahon AJ, Fischbacher CM, Frame SH, MacLeod MCM. Impacr of
laparoscopic cholecystectomy; a popularion-based study. Lancet 2000;
356(9242):1632.
68. Margolin DA. Beck DE. Surgical therapy for ulcerative colitis. Ostomy
Q I 997;34( I ):36.
69. Wrighr KD. ColosrolllY. In K Boyden, D Olendorf (eds), Gale Encyclopedia of Medicine. Farmingron Hills, MI: Gale Group, 1999;760.
70. Madick SS. Sromach rumors and gamic surgery. AORN J 1999;69(4):
824.
71. Mergener K, Baillie J. Chronic pancreariris. Lancer 1997;350(9088):
1379-1385.
72. Dean E. Oxygen transport deficits in systemic disease and implications
for physical rherapy. Phys Ther 1997;77(2):187-202.

9
Genitourinary System
Jaime C. Paz
lntroduction
The regulation of fluid and electrolyte levels by the genitourinary system is an essen rial component to cellular and cardiovascular function.
Imbalance of fluids, electrolytes, or both can lead to blood pressure
changes or impaired metabolism that can ultimately influence the
patient's activity tolerance (see Appendix II). Genitourinary structures
can also cause pain that is referred to the abdomen and back. To help
differentiate neuromuscular and skeletal dysfunction from systemic
dysfunction, physical therapists need to be aware of pain referral patterns from these structures (Table 9-1). The objectives for this chapter are to provide the following:
1.
A basic understanding of the structure and function of the
genirourinary system
2.
Information about the clinical evaluation of the genitouri-
nary system, including physical examination and diagnostic studies
3.
A basic understanding of the various diseases and disor-
ders of the genitourinary system
557



558
AClITE CARE HANDBOOK FOR PHYSICAL THeRAPISTS
Table 9-1. Segmental lnnervarion and Pain Referral Areas of the Urinary System
Segmental
Structure
Innervation
Possible Pain Referral Area
Kidney
Tl0-L l
Lumbar spine (ipsilateral flank)
Upper abdomen
Ureter
T I 1-L2, 52-54
Groin
Upper and lower abdomen
Suprapubic region
Scrotum
Medial and proximal thigh
Thoracolumbar region
Urinary bladder
TII-L2,52-54
5ac,,1 apex
Suprapubic region
Thoracolumbar region
Source: Wirh permission from we Boisson:Hlir, C B..1SS. Parhological origins of trunk and
neck pain: part I. Pelvic and abdominal visceral disorders. J Orthop Phys Ther 1990; 12: 194.
4.
Information about the management of genitourinary dis-
orders, including dialysis therapy and surgical procedures
5.
Guidelines for physical therapy intervention in patients
with genitourinary diseases and disorders
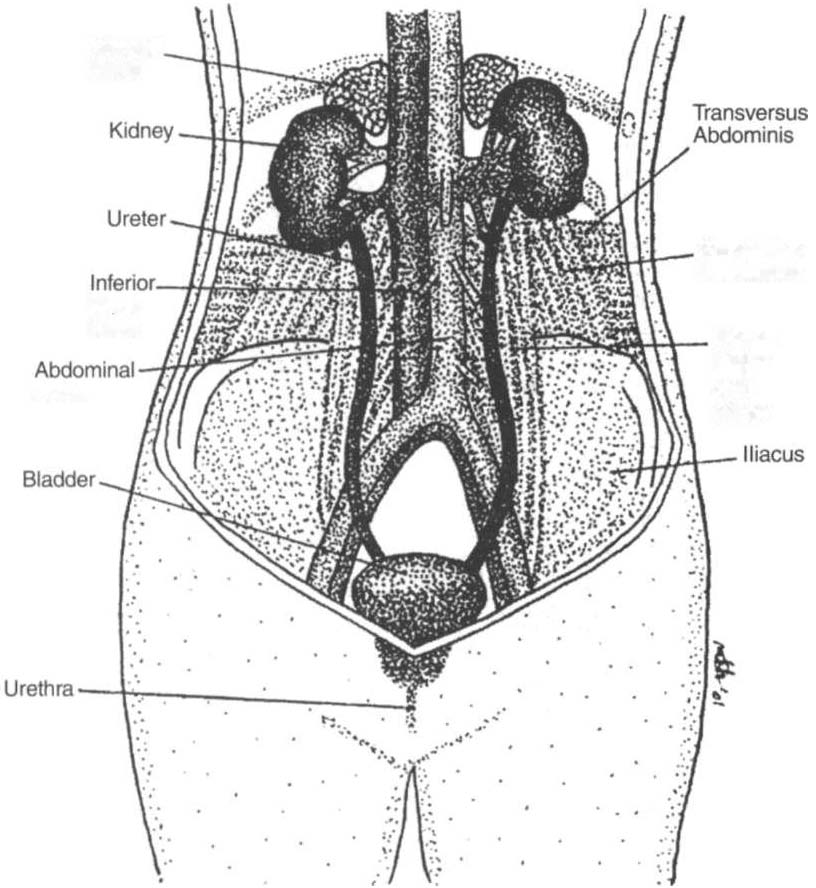
Structure and Function
The genitourinary system consists of two kidneys, two ureters, one
urinary bladder, and one urethra. The genitourinary system also
includes the reproductive organs: the prostate gland, testicles, and
epididymis in men and the uterus, fallopian tubes, ovaries, vagina,
external genitalia, and perineum in women. Of these reproductive
organs, only the prostate gland is discussed in this chapter.
The anatomy of the genitourinary system is shown in Figure 9-1.
An expanded, frontal view of the kidney is shown in Figure 9-2. The
structural and functional unit of the kidney is called the /lephro/l. The
nephron is located in the renal cortex and the medulla and has twO
parts: a renal corpuscle and a renal tubule. There are approximately 1
million nephrons in each kidney. Urine is formed in the nephron