The End of Diabetes (3 page)
Read The End of Diabetes Online
Authors: Joel Fuhrman

Â
I have been on your plan for two years and am really happy with the results. I am at my ideal weight with about 10 percent body fat. A couple of years ago I was 190 pounds with high cholesterol. My insulin was at 30u Lantus and Humalog on a sliding scale but often like 6u per meal. Following your advice I dropped the weight to 170, my cholesterol is awesome now, and blood pressure and lipid profiles are great! Now my Lantus is 10u and I am on Novolog, two or three units per meal.
When I was diagnosed in my teens, my doctor said there were two ways to look at the diagnosis:
1. as the end of my health forever or
2. an opportunity to gain an understanding of my body and how it works and become healthier than ever
I tried to take the latter road, and now, at age thirty-four, I think I am finally realizing that potential. Your writings were the suit of armor I needed in the fight all these years. Thanks again for everything.
âTony Gerardo
Several studies illustrate the dangers of giving insulin to the adult diabetic. In one such study, when diabetic patients were given insulin, compared to those given metformin (Glucophage), the risk of death from heart attacks tripled.
5
The negative effects of insulin are related to both the systemic metabolic abnormalities from excessive insulin and the direct pro-atherogenic effects of insulin on the endothelial lining of blood vessels that promotes atherosclerosis.
6
The more insulin that is needed, the more dangerous plaque is promoted, especially when the amount of circulating insulin is high. Extra insulin and high blood sugar levels also raise cholesterol, promote fat deposition, and damage the body. With this in mind, it should be clear that while the SAD, which has spread to all industrialized nations, is dangerous for everyone, it is particularly deadly for diabetics. Diabetes is not a death sentence, but we can't keep following conventional medicine and dieticians' advice or the excessive insulin and overuse of other medications they call for.
The negatives of overprescribing insulin are not limited to weight gain and heart disease. The connection between diabetes and cancer is thought to be due at least in part to insulin therapy. A new review that analyzed data from several studies found that diabetic patients are 30 percent more likely to develop colorectal cancer, 20 percent more likely to develop breast cancer, and 82 percent more likely to develop pancreatic cancer.
7
I am certain that by using insulin in small physiological amounts in type 1 diabetics, whose insulin needs would be low on my nutritarian diet, the metabolic negatives and the increased risk of cancer from insulin would
not
be noted. These negatives are the result of the excessive use of insulin necessitated by the SAD and the standard diabetic diet.
When type 1 diabetics follow the Eat to Live approach, it is possible to prevent many of the complications that can accompany the disease. As discussed, a normal life and life span are well within reach. Type 1 diabetics will still require insulin, but for almost all patients, the insulin dosages required will be greatly reduced, and they will require only the amount of insulin that a person's pancreas would secrete if eating healthfully and nondiabetic, so no damage will ensue because they are not requiring abnormally high amounts of insulin.
Specifically, if type 1 diabetes is well managed, there will be many benefits:
Â
â¢Â No highs or lows in blood sugar
â¢Â Less insulin useâmost typically, dose is cut by half
â¢Â Normal, stable body weight
â¢Â Normal life span, without diabetic complications
Â
The key formula to remember here is that favorable glucose levels + excellent nutrition = a healthy and long life. If you or someone you love has type 1 diabetes, please read this book. I promise that it can save lives; I have seen it happen.
Â
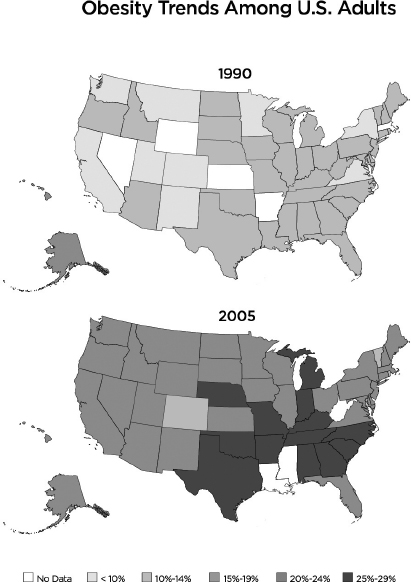
The Dramatic Increase in Type 2 Diabetes: A Tragic Phenomenon
Type 2 diabetes occurs in approximately 3 to 5 percent of Americans under fifty years of age and increases to 10 to 15 percent in people over fifty. More than 90 percent of diabetics in the United States are type 2 diabetics. Sometimes called adult-onset diabetes, this form of diabetes occurs most often in people who are overweight and who do not exercise sufficiently. The explosion in the occurrence of diabetes in the last twenty-five years in America parallels the skyrocketing number of overweight people.
Type 2 diabetes almost never occurs in people who eat healthy, exercise regularly, and have a low body fat percent. The disease hardly existed in prior centuries when food was not so abundant or when high-calorie, low-nutrient food was not available. It is also more common in people of Native American, Hispanic, Indian, and African-American descent, though no background is immune to the effects of a diabetes-inducing diet. Worldwide, diabetes is exploding as populations in all corners of the globe are being exposed to processed foods for the first time in human history. The development and abundance of processed foods in the world's food supply combined with more sedentary jobs has created an explosion of obesity, diabetes, and heart disease. Most countries have attempted to solve this problem with medications for diabetes, high blood pressure, and high cholesterol. Invasive medical procedures and surgeries are used at a substantial expense but without significant life span enhancements or benefits to society.
In the United States, being overweight is the norm, and almost all adults eventually take prescribed medications for their heart, diabetes, cholesterol, or blood pressure. In fact, 51 percent of those over the age of 65 take five or more prescription drugs a day! The number of obese Americans is higher than the number of those who smoke, use illegal drugs, or suffer from other physical ailments. Obesity is a major risk factor associated with highly prevalent serious diseases such as heart disease, cancer, and diabetes. It is what we eat that creates these diseases and fuels out-of-control medical costs. Even five extra pounds on a normal body frame can lead to diabetes.
Research shows that excess body fat is the most significant cause of type 2 diabetes. Through working with thousands of patients, I have observed with consistency that losing body fat in conjunction with maintaining high levels of micronutrients in the body's tissues will reduce the need for medications and, in most cases, reverse type 2 diabetes for good. As we'll explore in detail throughout this book, scientific studies show it is not just the weight loss but also the cell's exposure to a favorable micronutrient environment that enable recovery. Many of my patients recover from their diabetes before most of their weight has been lost. The cells become more responsive to insulin when the body is not burdened with excess fat, and the high level of micronutrients in the tissues enables the beta cells that have pooped out from struggling to produce extra high levels of insulin for years to reclaim lost function.
Because of its slow onset and the fact that it can usually be controlled with diet, type 2 is considered a milder form of diabetes, sometimes developing over the course of several years. The consequences of uncontrolled and untreated type 2 diabetes, however, are just as serious as those for type 1. Heart attacks, infections, amputations, blindness, and strokes are possible, but unlike type 1, type 2 diabetics can almost all come off insulin and other medications if they take off the excess weight.
Â
Prevalence of Diabetes Worldwide
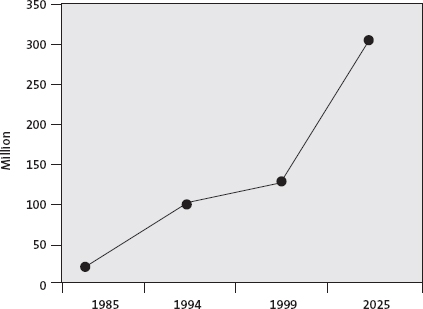
Diabetes isn't just about elevated blood sugar levelsâwhich pose immediate threats including blurred vision, drowsiness, confusion, and vomitingâit's about every other long-term condition and complication it creates as well. It can take a severe toll on the health of a diabeticâincreasing not only the risk of heart attacks and strokes but also of depression and cancer.
8
Â
What a Type 2 Diabetic Can Expect
Specifically, if type 2 diabetes is well managed with exercise and superior nutrition, there will be many benefits:
Â
â¢Â No highs or lows in blood sugar
â¢Â Reduction of medications by an average of 50 percent in the first week, more in the first month, and most typically 100 percent within six months
â¢Â Need for insulin is eliminated, usually within the first week
â¢Â Normal, lean, and stable body weight
â¢Â Normal life span, without complications
â¢Â Reversal of diabetes and prevention of diabetes-related complications
Â
The goal is to reverse diabetes to the point of becoming nondiabetic again, meaning ideally that your glucose levels run below 100 without medications. Be aware, though, that once you've been diabetic, the tendency to become diabetic again remains if you regain weight or go back to unhealthy eating. This is a new diet style and lifestyle forever.
You can anticipate your blood sugar falling with this diet and lifestyle plan. As discussed earlier, you will be able to reduce your medications. Err on the side of too little medication, not too much. Prevent the occurrence of hypoglycemic episodes with good communication with your physician and careful use of minimal medications.
If your blood glucose has been elevated for a while, even as your blood sugar approaches the normal range, you could feel somewhat ill as the body gets accustomed to experiencing normal blood glucose levels. Nevertheless, when on diabetic (glucose-lowering) medications, especially insulin and sulfonylureasâAmaryl (glimipiride), Diabenese (chlorpropamide), Glucotrol (glipizide), Diabeta, Glynase (glyburide), Actos (pioglitazone), Avandia (rosiglitazone)âit's important to check your blood sugar frequently during the first week to make sure you are not being overmedicated. Glucophage (metformin) is a commonly used oral diabetes medication that does not cause the blood glucose to drop too low and does not cause weight gain, so this is the preferred medication to remain on, if one is needed.
Snacking to prevent a hypoglycemic reaction from the overuse of medication is poor medical management and should not happen. Medications should be reduced in time so this never occurs. I tell patients starting this program that if a blood sugar reading is below 120, it is time for the next round of medication reduction. It is better to be undermedicated slightly, to prevent the need to treat hypoglycemic events, than it is to be overmedicated. If the diabetic patient experiences hypoglycemic episodes and extra snacking is required to bring the glucose up, then the physician overmedicated the patient and did not do his job correctly.
The ADA diet uses the diabetic exchange list to help diabetics create what they call balanced meals. This exchange diet divides foods up into groups based on similarities in nutrient content and includes starches, fruits, milk, vegetables, meats, fats, sweets, and other carbohydrates. It looks to make meals that are based on a preconceived notion that balancing an equal amount of fat, carbohydrates, and protein at each meal is favorable. It then allows exchanges based on the amount of calories from that macronutrient. For example, in the starch group, one slice of toast can be exchanged for a half cup serving of cooked oatmeal.
Because the foods the diet is designed with are inherently poor in fiber, micronutrients, and resistant starch, they fuel an obsession with food because the dieter is never satisfied. This continual struggle with dieting and trying to maintain small portion sizes of foods that do not biologically fill you up rarely works. Even in controlled dietary studies in which calories are carefully monitored, the results are relatively poor simply because the American dietary standard is so poor and the ADA diet mimics this failed dietary pattern utilizing too much unhealthy, low-micronutrient foods. Researchers have also frequently noted the difficulties involved in the ADA plan, particularly the requirements to dramatically restrict portion sizes that most individuals simply cannot comply with long term.
9
An ADA sample breakfast meal may include two slices of toast with one teaspoon of margarine, a scrambled egg, three-quarters of a cup of unsweetened ready-to-eat cereal with one cup of nonfat milk, and a small banana. Another breakfast choice on the 1,800-calorie ADA diet may include two four-inch whole wheat pancakes with two tablespoons of light pancake syrup, one teaspoon of margarine, one cup of sliced strawberries, one-quarter cup of low-fat cottage cheese, and one cup of nonfat milk. These sample meals are a formula for disaster for diabetics. In order to get the glucose controlled after consuming all those low-fiber carbohydrates, an excessive amount of diabetes medication will have to be prescribed, which will lead not only to highs and lows but also potentially to hypoglycemic episodes. Then diabetic patients are instructed to snack to prevent the low blood sugar results of the medication, further impeding their possibility of dropping the excess body fat. The additional side effects and weight gain from the medications just lead to a worsening of the diabetes. The focus with standard care is on the glucose level and maintaining the right amount of medication to optimally stabilize the glucose. It misses the boat, though, because it fails to focus on the health and weight of the person first, and the miraculous health and weight loss benefits of the right dietary pattern based on greens, beans, mushrooms, onions, tomatoes, peppers, berries, intact grains (not just whole grains), seeds, and nuts.