The Rise and Fall of Modern Medicine (45 page)
Read The Rise and Fall of Modern Medicine Online
Authors: James Le Fanu

Among those interested in solving the problem was Ancel Keys, the forty-year-old Director of the Laboratory of Physiological Hygiene at the University of Minnesota, who, at the close of the war, turned his attention to investigating why so many middle-aged men were dying from heart attacks. His particular scientific interest was nutrition, and so naturally enough he focused his attention on the chemical cholesterol present in the atheroma of the arteries. The main source of cholesterol is the liver, from where it is released into the bloodstream to fulfil its indispensable role as an integral part of the walls lining the cells, as well as being the precursor of many important hormones, including testosterone in the male and oestrogen in the female. Perhaps, Keys speculated, the other source of cholesterol â in food such as eggs and avocados â might, in combination with other fats, force up its level in the blood, which would then infiltrate the artery walls to form the
atheroma that appeared to be implicated in heart attacks. It was not an original idea, but Ancel Keys was to pursue it so vigorously over the next years as essentially to make it his own.
9
Firstly, it was necessary to know more about the predisposing factors for a coronary, so Keys set up a âprospective' study, on the lines of Bradford Hill's famous Doctor Study into smoking, involving almost 300 businessmen from his home town of Minneapolis. They were weighed and measured, their cholesterol levels monitored and their blood pressure recorded and their fate followed over the succeeding twenty-five years. From this it emerged there were three main ârisk factors' â smoking, raised blood pressure and a high cholesterol level â that together markedly increased the subsequent risk of a coronary.
10
Next he investigated the effect of different types of diet, and this time he turned to the local mental asylum. Over a period of several years thirty patients with schizophrenia were subjected to a wide assortment of diets containing various amounts and types of fat: cocoa butter, corn oil, beef fat, rape seed oil, and so on.
11
From this it emerged that it was possible to lower the cholesterol level in the blood by lowering the amount of saturated fat (as in meat, milk and dairy products) and increasing the amount of polyunsaturated fat (as in vegetable oils), but it was not easy. Substantial changes were required because, as already pointed out, the survival of the human organism requires that the â
milieu intérieur
' â its physiological functions (such as the level of cholesterol in the blood) â should not be sensitive to modest changes in the â
extérieur
' such as the amount and type of food consumed. Rather, many âfeedback' mechanisms ensure the cholesterol levels stay at a steady state, so if the amount of fat in the diet is reduced, the liver compensates by increasing the amount of cholesterol it makes. There was another problem. The role of fat consumption in the heart
disease epidemic would have been more straightforward had the Minnesota businessmen with high cholesterol levels been at âgreater risk' because they consumed more saturated fat. But this was not the case. Their dietary pattern was no different from that of anyone else.
It remained a puzzle until, almost inadvertently, Keys stumbled on what he believed must be the answer while on a trip to Rome in 1951 to chair a United Nations committee, where the Professor of Physiology at the University of Naples pointed out that heart disease was ânot a problem' in his city. He invited Keys to come and see for himself, and the following year he and his wife Margaret (a trained biochemist who specialised in measuring cholesterol levels in the blood) arrived in Naples and set up their cholesterol-measuring equipment. Soon their Neapolitan friends were bringing in workers from the neighbourhood. Their cholesterol levels turned out to be one-third lower than those of the businessmen they had been studying back in Minnesota. The explanation had to be the Neapolitan diet:
There is no mistaking the general picture â a little lean meat once or twice a week was the rule, butter was almost unknown, milk was never drunk except in coffee or for infants, âcolazione' on the job often meant half a loaf of bread crammed with baked lettuce or spinach. Pasta was eaten every day, usually also with bread (no spreads) and a fourth of the calories were provided by olive oil and wine. There was no evidence of nutritional deficiency but the working-class women were fat.
Over the next few years Keys travelled the world investigating the relationship between diet and coronary heart disease in
different countries, culminating in 1956 with visits to the city of Fukuoka in Japan and the province of North Karelia in Finland. The Japanese famously enjoy a low-fat diet with little meat and dairy products but many fish and pickled foods, so the blood samples analysed by Margaret Keys from Japanese farmers, clerks and coalminers revealed, by now predictably enough, a low cholesterol level in the blood. Meanwhile a cardiologist, Paul White, who was accompanying them, âspent weeks trying to find a case of coronary thrombosis in the big medical school hospital, district hospitals and private clinics'. Later the same year Keys arrived with his entourage in North Karelia on the Finnish border with Russia:
The first village had an infirmary with six beds for male patients. One was a young man who had been bitten by a bear. A second had cancer of the lung and the third was occupied by an old man wheezing with asthma. The other three patients had coronary heart disease. Later we went into the woods to have a sauna with some lumberjacks. Two of them confessed to being slowed up by angina, but even more interesting was a glimpse into the local eating habits, the favoured âafter-sauna' snack was a slab of full-fat cheese the size of a slice of bread on which was smeared a thick layer of âthat good Finnish butter'.
12
There remained the possibility that the marked discrepancy in cholesterol levels and susceptibility to heart disease might be due to genetic differences between the Japanese and the Finlanders. The following year Keys tackled the question in a typically ingenious way. In the 1950s the Japanese economy was still devastated by the effects of the Second World War, encouraging many Japanese to migrate first to Hawaii â a sort of
cultural halfway house between Japan and America â and then to Los Angeles. Keys proceeded to test Japanese migrants in Hawaii and Los Angeles and then compared the results with those they had obtained from the indigenous Japanese of Fukuoka the previous year. There was a clear gradient: as the Japanese became progressively more Westernised, so their cholesterol levels rose or, as Keys put it, âthe conclusion seemed to be inescapable â the proportion of calories provided by saturated fat (meat, milk and dairy products) is an important factor in the frequency of coronary heart disease'.
13
Thus was born the diet-heart thesis, the answer to the problem that Sir Maurice Cassidy admitted ten years previously âI cannot solve': too much fat in the diet pushes up the cholesterol level in the blood, which infiltrates and narrows the walls of the coronary arteries, resulting in a heart attack.
(From R. E. Stallones, â
The Rise and Fall of Ischaemic Heart Disease
', Scientific American, 1980, Vol. 243, pp. 43â9.)
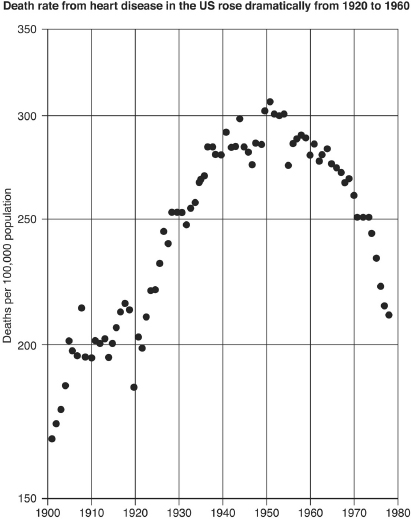
So by the mid-1950s Ancel Keys had become convinced for good reasons that his original hypothesis of the epidemic of coronary heart disease as âa nutritional disorder' â because of excess consumption of saturated fat â must be correct. But when, in 1957, the American Heart Association (AHA) invited a group of heart specialists to evaluate his theory they were unable to endorse it. They noted that within the United States an individual's food preferences neither predicted the level of cholesterol in their blood nor their subsequent risk of heart disease, hence food could scarcely be a determinant factor. They then turned to the two major weaknesses of Keys's theory. First, it failed to account for the striking âepidemic' pattern of heart disease (see opposite), increasing exponentially year by year from the 1920s to become, by the early 1950s, much the commonest cause of death in middle-aged men. Clearly this dramatic rise in heart disease had not been paralleled by the necessary and substantive changes in the pattern of food consumption. Second, Keys had failed to account for the central feature of a coronary thrombosis â the clot or thrombus in the coronary artery that, by blocking the blood supply to the heart muscle, caused the sudden, dramatic symptoms of a heart attack. As one of his most
distinguished critics, Sir George Pickering, Regius Professor of Medicine at Oxford, was subsequently to observe: â[Keys's thesis] assigns a minor role, in fact almost an afterthought, to the event that determines life or death.'
14
These reservations all pointed to a rather different interpretation of Keys's findings: a âhigh-fat' diet along with smoking and raised blood pressure might be a
contributory
but not a
determinant
factor in the rise of heart disease. The Western diet certainly seemed to explain the higher average cholesterol levels in the West compared to other countries such as Japan, which in turn might predispose to both the narrowed arteries and the thrombus. Further, within Western societies, individuals with a genetic predisposition to a higher cholesterol level, such as the Minnesota businessmen, would be at increased risk. But diet could not begin to explain the dramatic rise in heart disease, as this would have required truly monumental increases in fat consumption in the United States that clearly had not happened. Keys's explanation, self-evident as it might seem, failed Bradford Hill's requirement that epidemiological evidence be âinternally coherent', that it hangs together in such a way that from whatever angle the question is examined, it points to the same conclusion. Keys was half right â heart disease does have âsomething to do with' cholesterol levels â but from the important point of view of doing something to prevent heart disease it was, regrettably, the wrong half. Further, it would be quite unrealistic to expect people to make the major changes required in switching from a Western-style to a Mediterranean- or Japanese-style diet, when the resultant fall in cholesterol would only indirectly reduce the risk of a heart attack. A subtle point, perhaps, but sometimes subtlety can be important. And so the AHA committee concluded that âthe evidence does not convey any specific implications for drastic dietary changes'.
15
The verdict of the AHA was a serious blow. It conveyed the impression that Keys's scientific work over the previous ten years, impressive as it undoubtedly was, nonetheless could not sustain the interpretation he had placed on it. Keys, it would seem, was just one of many scientists who over the years had backed the wrong horse. Nor was he the only person to be discomfited. The careers of several other scientists who had rallied to his banner would similarly founder in the absence of official endorsement. The most prominent of these, and destined to become Keys's lifelong friend, was Jeremiah Stamler of Chicago University. In 1957, at the time of the publication of the AHA report, Stamler was about to launch the Coronary Prevention Evaluation Programme, whose purpose, as its name implies, was to demonstrate that heart disease was indeed preventable by encouraging people to take more exercise, stop smoking and change to a âhealthy' diet.
16
The AHA's failure to endorse the need for âdrastic dietary change' placed him in the same invidious position as Keys â vulnerable to the charge of dietary crankery, someone whose ideas were outside the mainstream of medical thinking.
Clearly the AHA had to be persuaded to change its mind. It took some time but within a couple of years the membership of the relevant committee had been reconstituted to include both Keys and Stamler. Its next report, predictably, was very different in tone and content from the first, running to a mere two pages, thus omitting any discussion of the substantial problems of Keys's thesis. Reversing the previous conclusion, it recommended that people should indeed reduce the amount of fat in their diet in anticipation of reducing the risk of heart disease while admitting there was, as yet, âno final proof â.
17
The reversal of the original committee's conclusion might seem a trivial matter but, over the next four decades, it would profoundly
influence public beliefs, government policy and the practice of medicine.
Keys and Stamler then had a stroke of luck. The main contending explanation for heart disease â that the most important factor was the clot or thrombus in the coronary artery â was undermined with the publication in 1964 of an authoritative study evaluating the benefits of blood-thinning drugs (anticoagulants), which should, if the clot was the critical factor, have had a major impact on the risk of a heart attack. These drugs, it emerged, could indeed reduce the risk of a heart attack by reducing the âclotability' of the blood, but this benefit was equally balanced by an increase in the numbers in whom the anticoagulants had also resulted â as they were likely to â in a fatal haemorrhage into the brain.