Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (1124 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
8.37Mb size Format: txt, pdf, ePub
Renin-producing tumors of the kidney
TABLE 16–66. Differentiation of Primary and Secondary Aldosteronism Based on Blood Tests and Clinical Symptoms
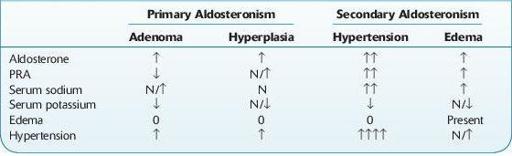
↑, increased; ↓, decreased; N, normal.
Decreased In
Other books
After Dachau by Daniel Quinn
The Confidence Woman by Judith Van Gieson
Tanya Tania by Antara Ganguli
Pulling The Dragon's Tail by Kenton Kauffman
He Owns My Wife by Tinto Selvaggio
Widow Woman by Patricia McLinn
The Seven Daughters of Eve by Bryan Sykes
Inside the Gender Jihad: Women's Reform in Islam by Amina Wadud
The Possibility of an Island by Houellebecq, Michel, Gavin Bowd
The App Generation by Howard Gardner, Katie Davis