Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (190 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

Assess the patient for alcohol and drug abuse; consider
drug screen.
AFP
to assess the patient for liver tumor and ascites.

Assessment of response to HCV antiviral therapy
: The goal of antiviral treatment is a sustained virologic response (SVR), which is defined as undetectable HCV RNA 6 months after the end of therapy.
Patient factors
: Pretreatment factors associated with a lower rate of SVR include inability to comply with the treatment regimen, diabetes or insulin resistance, increased body weight, older age, increased portal hypertension or abnormal liver histopathology (fibrosis, cirrhosis, steatosis), statin use, increased triglyceride or HDL, and decreased LDL.
Baseline
: Patients with pretreatment HCV viral loads >800,000 IU/mL are less likely to achieve SVR, compared to patients with lower baseline viral loads.
Rapid virologic response (RVR)
: Monitoring HCV viral load should begin as early as 2–4 weeks after initiation of antiviral therapy with pegylated interferon/ribavirin or triple therapy (e.g., pegIFN/RBV plus telaprevir or boceprevir). The rate of fall of the HCV viral load is an important predictor of SVR, especially for genotype 1 virus. Patients with negative HCV RNA at 4 weeks have high (>90%) rates of SVR and may be eligible for a shortened duration of therapy.
10
reduction compared to baseline; SVR >70% is seen in patients with undetectable HCV RNA at 12 weeks.
Patients who do not show a >2 log
10
reduction in HCV viral load, compared to their baseline, are unlikely to achieve an SVR (<2%).
TABLE 5–11. Comparison of Types of Hepatitis D Virus (HDV) Infections
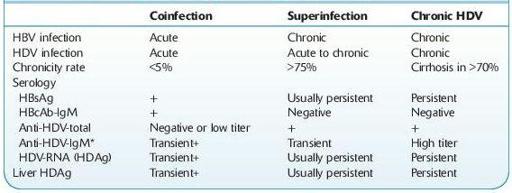
+, Positive.
*Decrease in anti-HDV-IgM usually predicts resolution of acute HDV. Persistent anti-HDV-IgM typically predicts progression to chronic HDV infection. High titer correlates with active liver inflammation.
TABLE 5–12. Serologic Diagnosis of Hepatitis B Virus (HBV) and Hepatitis D Virus (HDV)
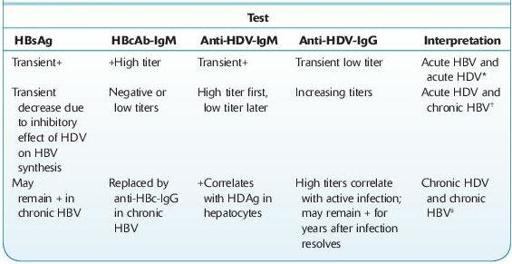
+, Positive.
*Clinically resembles acute viral hepatitis; fulminant hepatitis is rare, and progression to chronic hepatitis is unlikely. If HBV does not resolve, HDV can continue to replicate indefinitely.
† Clinically resembles exacerbation of chronic liver disease or of fulminant hepatitis with liver failure.
‡ Clinically resembles chronic liver disease progressing to cirrhosis.