Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (543 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
3.56Mb size Format: txt, pdf, ePub
Focal nephritic: generally associated with inflammatory regions in less than one half of glomeruli. Patients often present with asymptomatic hematuria and proteinuria.
Causes
Renal: can be postinfectious (due to certain nephritogenic strains after streptococcal, staphylococcal, or pneumococcal infections, mumps, measles, chickenpox, hepatitis B and C) or due to MPGN or anti–glomerular membrane disease.
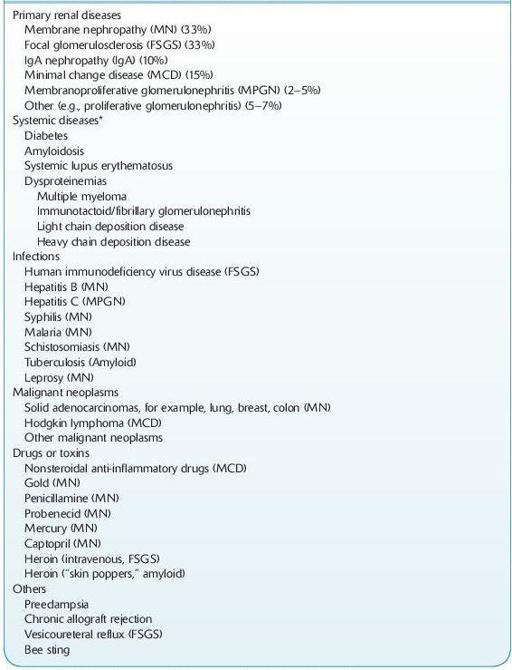
NEPHROTIC SYNDROME
This syndrome presents as heavy proteinuria, hypoalbuminemia, hyperlipidemia, lipiduria, and edema.
12-5
).
TABLE 12–5. Major causes of Nephrotic Syndrome
Other books
1.4 by Mike A. Lancaster
The Good Die Twice by Lee Driver
Death Screams by Tamara Rose Blodgett
Smooth Operator (Teddy Fay) by Woods, Stuart, Hall, Parnell
Chosen: Book 1 in the Ancients of Light series by Heather Fleener
Lafferty, Mur by Playing for Keeps [html]
Reed (The Love Family Series Book 4) by Allenton, Kate
First Verse (Second Verse Book 1) by Snow, Emily
House of Cards by Michael Dobbs
Give It All by Cara McKenna