Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (559 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
11.53Mb size Format: txt, pdf, ePub
This condition, which involves amyloid deposition in the kidneys, is one of the most frequent complications of AA, AL, and several hereditary forms of amyloidosis.
Who Should Be Suspected?
Candidates include patients with known systemic amyloidosis who develop proteinuria or, in the absence of this diagnosis, individuals with new-onset proteinuria, renal insufficiency, or nephrotic syndrome of unknown etiology.
Suggested Reading
Dember LM. Amyloidosis-associated kidney disease.
J Am Soc Nephrol.
2006;17:3458–3471.
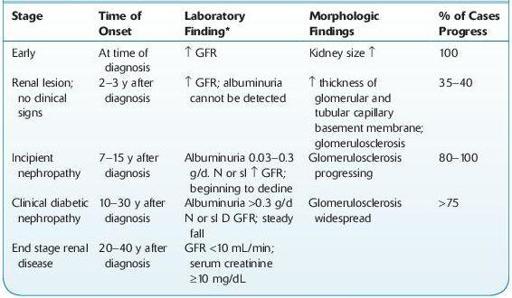
DIABETIC NEPHROPATHY
12-7
).
TABLE 12–7. Evolution of Renal Disease in Insulin-Dependent Diabetes Mellitus (IDDM)
Other books
The Beckoning Lady by Margery Allingham
At Wick's End (Book 1 in the Candlemaking Mysteries) by Tim Myers
The Courage Consort by Michel Faber
Knight Triumphant by Heather Graham
Stacey And The Mystery Of Stoneybrook by Ann M, Martin
Nowhere to Run by C. J. Box
TIMBER: The Bad Boy's Baby by Frankie Love
Lure of the Wicked by Cooper, Karina
All This Time by Marie Wathen
Queermance Anthology, Volume 1 by Lindy Cameron