Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (594 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
5.18Mb size Format: txt, pdf, ePub
It is clinically important to classify pleural and ascitic fluids into exudates and transudates because this is indicative of the underlying pathophysiologic process involved (Figure
13-1
). A transudate does not usually require additional testing, but exudates always do.
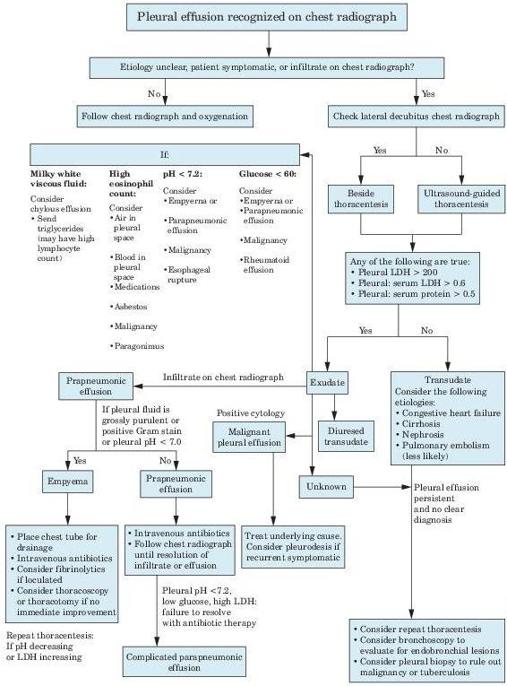
Figure 13–1
Algorithm for the workup of patients with pleural effusion. LDH = lactate dehydrogenase.
Transudate
Causes
CHF (causes 15% of cases); acute diuresis can result in pseudoexudate
Other books
A Cold White Fear by R.J. Harlick
From Here to Paternity by Jill Churchill
09 The Clue at Black Creek Farm by Carolyn Keene
When You Are Engulfed in Flames by David Sedaris
Her: A Memoir by Christa Parravani
The Mirrored World by Debra Dean
Denise's Daily Dozen by Denise Austin
The Standing Dead - Stone Dance of the Chameleon 02 by Ricardo Pinto
Brave the Storm, Season 2, Episode 3 (Rising Storm) by Lisa Mondello
Mission to Paris by Alan Furst