Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (65 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
9.94Mb size Format: txt, pdf, ePub
Definition
Hyperlipidemia is an elevation of lipids (cholesterol, cholesterol esters, phospholipids, and triglycerides) in the bloodstream; is a risk factor for coronary heart disease (CHD); and promotes atherosclerosis. Lipids are transported as lipoproteins in the body; there are five major types: chylomicrons, VLDLs, intermediate-density lipoproteins (IDLs), LDLs, and HDLs. The protein portions of the lipoprotein are referred as apolipoprotein, of which there are six major classes (A, B, C, D, E, and H) and numerous subclasses (AI, AII, AIV, AV, B48, B200, CI, CII, CIII, and CIV).
3-2
).
3-3
).
TABLE 3–2 Diseases That May Cause Dyslipidemia and Associated Lipid Changes
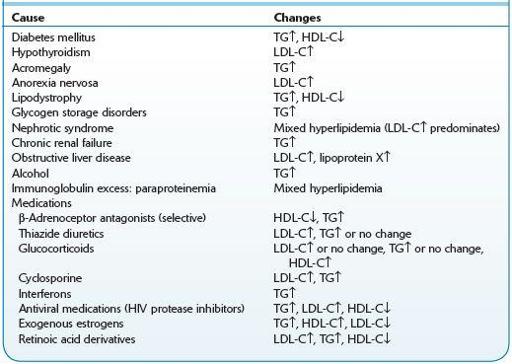
HDL-C, high-density lipoprotein–cholesterol; LDL-C, low-density lipoprotein–cholesterol; TG, triglyceride; ↑, increased levels; ↓, decreased levels.
TABLE 3–3 Classificationof Familial Dyslipidemias According to Predominant Lipid Abnormality and Etiology
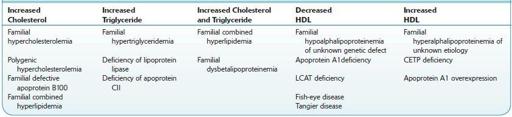
CETP,cholesterylestertransportprotein;HDL,high-densitylipoprotein;LCAT,lecithin–cholesterolacyltransferase;TG,triglyceride.
Low-risk persons: Further testing is not required if the HDL-cholesterol level is ≥40 mg/dL and TC is <200 mg/dL.
Other books
Titan (GAIA) by Varley, John
Equal Access by A. E. Branson
The Second Spy: The Books of Elsewhere: Volume 3 by West, Jacqueline
Death in a Funhouse Mirror by Kate Flora
Ransom Game by Howard Engel
Why We Buy by Paco Underhill
Gingham Mountain by Mary Connealy
Twisted Desire by Laura Dunaway
The House Above the River by Josephine Bell
Framed by C.P. Smith