Blood and Guts (18 page)
Authors: Richard Hollingham

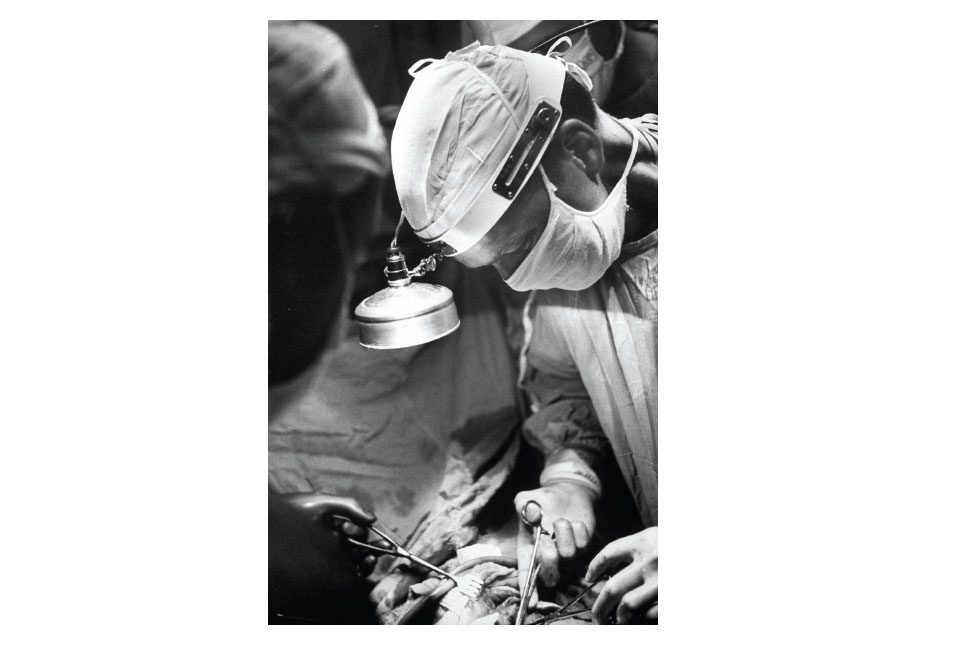
Walter Lillehei operating on a
beating human heart.
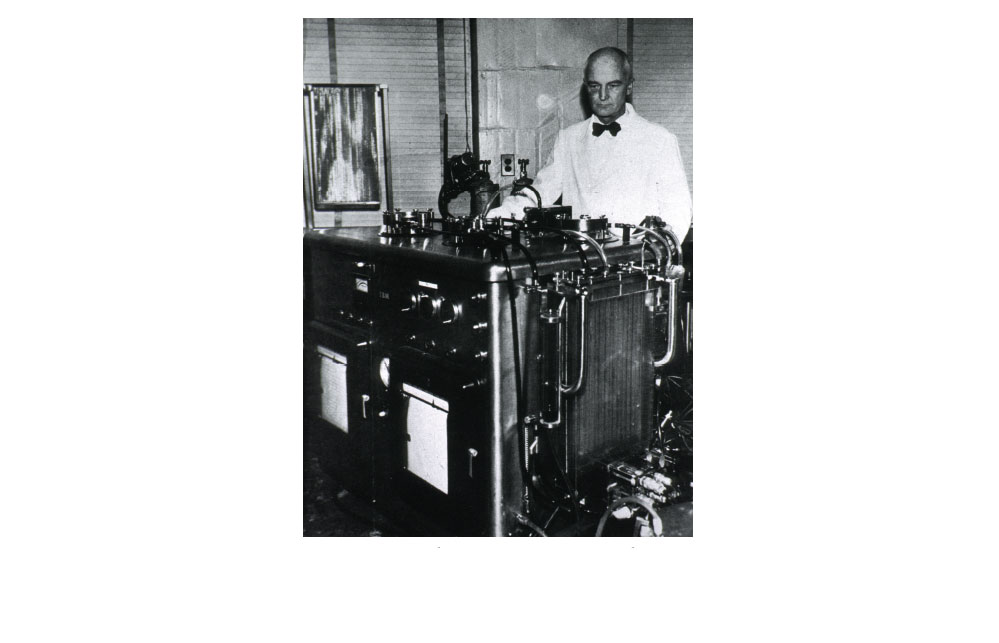
One of the few pictures ever taken
of John Gibbon with his fearsome looking
heart-lung machine. At the top left of the
machine is the screen where the blood
was oxygenated.

Christiaan Barnard with the world's first heart transplant patient, Louis Washkansky,
in 1967. The plastic sheet was used to help protect Washkansky from infection.
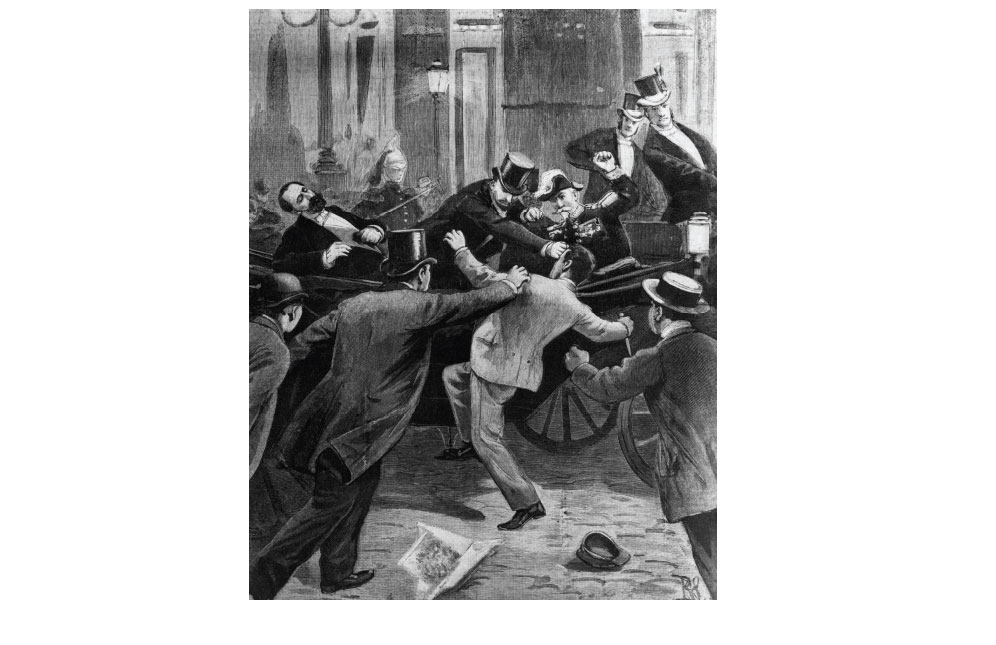
The dramatic assassination of
President Sadi Carnot on 25 June 1894.
The murderer is being grabbed by the
crowd as he attempts to make his escape.
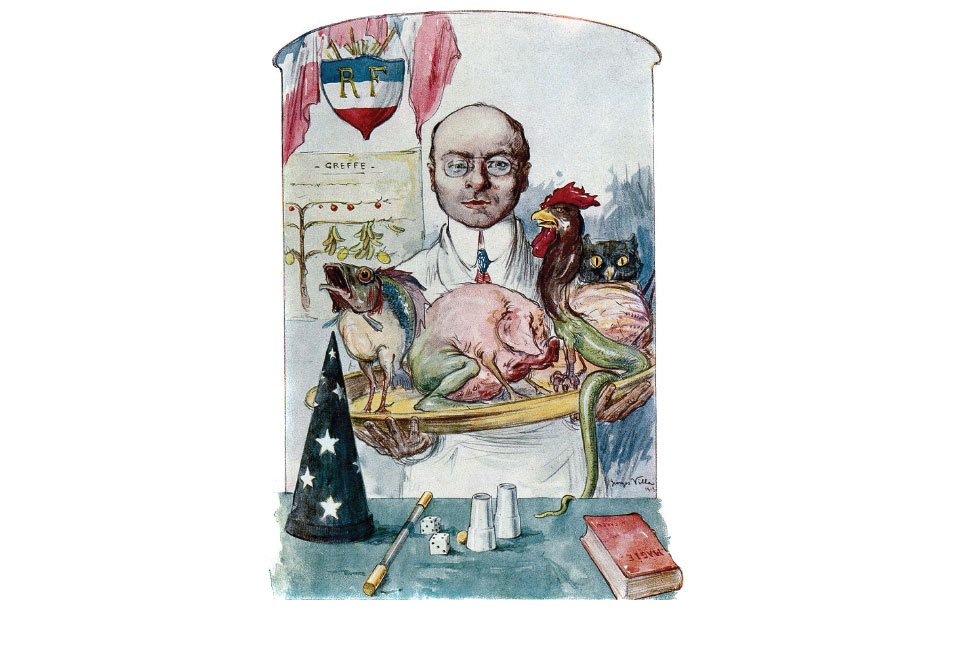
The weird and wonderful world of
Alexis Carrel in an illustration taken from a
French periodical. It's difficult to tell whether
they were proud of their countryman.
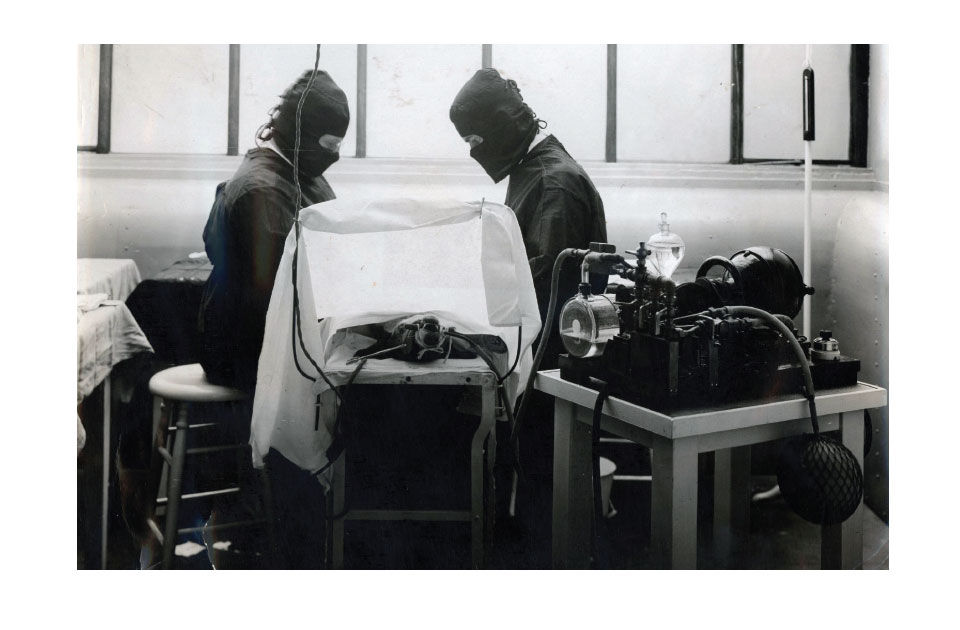
Another experiment in the laboratories of Alexis Carrel. Heaven knows what is
going on behind the sheet. This picture is undated, but was probably taken in the 1930s.
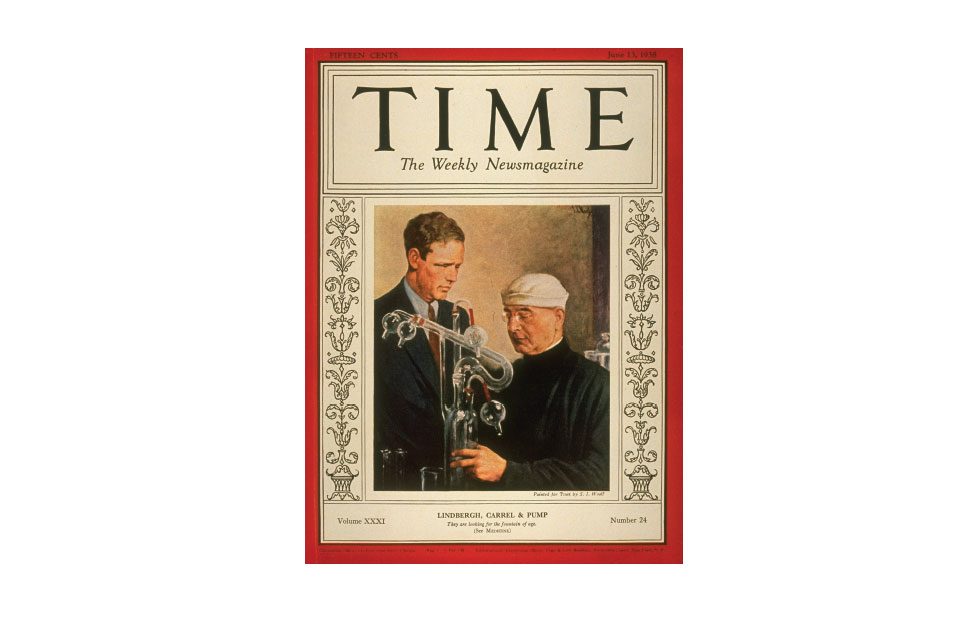
Alexis Carrel and
Charles Lindbergh make the
cover of
Time
magazine in
June 1938. Not long afterwards,
their reputations would go
into freefall.

The appalling result of Vladimir Demikhov's 1959 operation
to transplant the head of a puppy onto the head of another dog.

Richard Herrick is
wheeled out of hospital
by his identical twin
brother, Ronald, on
19 January 1955.
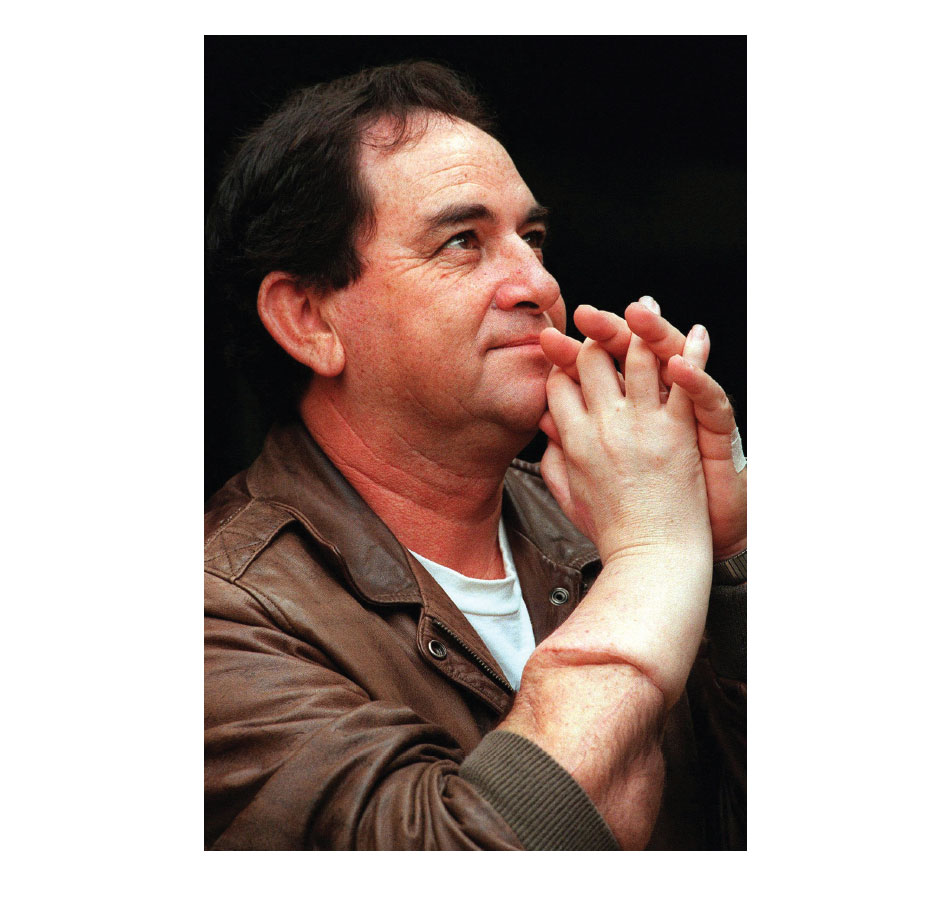
Clint Hallam enjoying the
use of his recently transplanted
hand in 1998. Even before
Hallam's body started to reject
the transplant, its appearance
was disconcerting.
DEAD MAN'S
HAND
THE STORY OF A TRANSPLANT
March 2000
From a distance, there was something odd about New Zealander
Clint Hallam. When he walked towards you it became obvious that
one arm was longer than the other. Up close the arm was even more
disturbing, verging on the grotesque. Anyone who saw his hand
would remember it for ever, perhaps in their nightmares.
Hallam recalls sitting in an aircraft next to a nice old lady. They
got talking. The lady recognized Hallam from somewhere, but
couldn't quite place him. Then she happened to glance down at his
right hand. Recoiling in shock, she pressed the call button to
summon the flight attendant and asked to be moved to another
seat. The lady turned to Hallam to apologize. She said she had nothing
against him personally, only she couldn't bear sitting next to
someone who was wearing a dead man's hand.
One of Hallam's close friends made a similar confession. Hallam
could never understand why, when they met, his friend would always
grasp Hallam's wrist rather than shake his hand. Hallam reckoned it
was an act of kindness, to avoid any risk of injury to his limb. When
he asked about it, his friend confessed to finding Hallam's hand
quite horrific. He wasn't the only one. The recipient of the world's
first hand transplant was beginning to realize that many people
found his new hand repulsive. Now, eighteen months after the
operation, even Hallam was beginning to have some doubts.
From the shoulder down, the upper part of Hallam's right arm
was perfectly normal. Its skin tone matched Hallam's dark complexion
and was covered in black hairs and dotted with freckles. Then,
just beyond the joint of the elbow, there was a sharp division where
the skin became pale and practically hairless. It was as if Hallam
was wearing a long white glove. There was a bulge – a swelling –
where the brown skin met the white. It was a long white glove that
didn't quite fit.
The underside of Hallam's lower right arm was bruised and
damaged. The skin was inflamed, raw and angry – as if he had been
burnt. Beyond the wrist the hands were similarly swollen. The skin
was peeling; there were ulcers and the flesh was shiny. It looked like
the outer layer of skin had been stripped away. When it came to the
fingers, the decay was even more pronounced. The fingertips were
crusty and sore, the yellow nails gradually separating from the flaking
skin underneath. Small wonder the woman on the plane chose
to move to another seat.
Hallam had received his hand transplant on 23 September 1998
at the Edouard Herriot Hospital in Lyon, France. The operation
took almost fourteen hours and was a brilliant technical achievement.
Earl Owen led a team of some the world's most experienced
transplant specialists from Australia, Britain, France and Italy.
France was chosen to host the operation because of its laws on organ
donation. There you have to opt out of donating your body to medicine,
rather than opting in. As a result, almost everyone who dies
becomes a potential donor, so many more donors are available –
perfect if you are waiting for a new arm and hand.
The donated limb came from that all too frequent source of
body parts – a motorcyclist. The limb was matched for blood type
and tissue type, but, as it turned out, not appearance.
The surgical technique used to join together Hallam's stump
and the dead motorcyclist's lower arm is known as microsurgery and
is fantastically intricate. The surgeons wore powerful magnifying
lenses and employed precise instruments, tiny needles and the
finest of threads.
First they joined together the two bones of the forearm to hold
the limb stable. Then they connected the blood supply – the arteries
and veins – to keep the tissue alive. Once the blood was flowing,
they stitched together the muscles and tendons and reconnected
the nerves. Finally, the surgeons were able to join together the skin.
At the inevitable press conference held shortly after the operation,
Owen described himself as 'very happy'. It was a moment of
surgical glory. 'We all have big smiles,' he said, and gave the operation
a fifty-fifty chance of long-term success. Others were equally
enthusiastic. Eminent British transplant surgeon Nadey Hakim
called it an 'incredibly exciting breakthrough,' adding, 'to see a
man restored with an arm is tremendously satisfying'.
The new arm had to be kept immobile for a few weeks while the
graft healed, but everyone was optimistic that the patient would
develop the full use of his limb. Hallam himself was overjoyed. It was
incredible to see fingertips at the end of his arm again. With a new
hand, he had been given a new life. It was a surgical miracle.
Hallam had spent years waiting for the operation. He lost his
original hand in an accident with a circular saw in 1984 while he was
serving time at a prison in New Zealand.
*
His severed hand had
been sewn back on, and although it looked OK, it had little function
and was all but useless. A few years later Hallam decided to get rid
of the hand altogether and opted instead for a prosthetic limb. This
hadn't worked out either, and he told the BBC that he had never
been able to accept having a lump of plastic attached to his arm. It
was not natural. Perhaps one day the technology would be available
for a hand transplant.
*
The circumstances of the injury remain somewhat vague. The surgeons who carried out the
1998 transplant operation were unaware that Hallam had sustained the injury in prison.
Hallam's somewhat chequered past was revealed by the media following the operation. This
did little to endear Hallam to the surgical team. Owen said later that although they had
conducted psychiatric tests, they should have looked more closely into Hallam's background.
However, a few months after the 1998 operation Hallam was
struggling to overcome his disappointment. It wasn't just the obvious
mismatch between his new arm and the old one, so much as the
practicalities. The new arm did not work very well. There was only
limited movement: Hallam could move the limb and bend his new
fingers to a limited extent, but he said he was almost more crippled
with the hand than he had been with a stump.
There was a marked contrast between Hallam's experiences and
the surgeon's rhetoric. They were claiming the operation as a great
success and told the media how Hallam could grab things, pick up a
glass and even write with a pen. They were also pleased that he could
feel pain and temperature on both sides of the new grafted hand.
But they weren't the ones who had to deal with the side effects.
To avoid the transplanted limb being rejected by his body's
immune system, Hallam had to take a cocktail of different drugs.
There could be eleven tablets to swallow in the morning, four at
lunchtime and eleven more in the evening. The exact amount
varied from week to week, but Hallam was usually being prescribed
some combination of steroids, anti-rejection tablets and immuno-suppressants
– drugs that, as the name suggests, suppressed his
immune system. He was also taking pills to help his fingernails
recover. Every day he had to count out the various tablets to make
sure he didn't take too many or too few. The pills were keeping his
arm alive, but they were also having other effects. Hallam had
started to develop diabetes and needed to take insulin to control his
blood sugar. Physically, he was also changing. Hallam was used to
keeping fit and had been in reasonably good shape. Now he found
he was growing breasts. Worse, the powerful drugs increased his risk
of developing cancer.
And it was not just the physical limitations that were taking their
toll. Hallam was beginning to realize that there was a psychological
price to pay for having a dead man's hand attached to his body.
Aside from the mental anguish for any man of growing breasts, the
transplant increasingly looked and felt like it did not belong. Other
people would comment, saying how white the transplant looked, or
how the new hand was smaller than the other one. Hallam realized
how angry he was with the doctors for not waiting for a hand
that was better matched. It was as if, he said, they were more interested
in the transplant than the person. He had dreamt for years
of having a new hand, but the reality was proving increasingly
uncomfortable. What happened next became inevitable.
By 2001, Hallam had begun to take fewer and fewer of his
prescribed drugs. Every time he got sick his immune system struggled
to cope, so he decided the answer was to cut down on the
immuno-suppressants, but the effect on his hand was hideous.
Attacked by his own body's immune system, the limb had all but
died; the flesh was rotting away on the end of Hallam's arm. He
had lost all feeling; it was a wonder the infection hadn't spread to
other parts of his body. Hallam told the BBC he felt 'mentally
detached' from the hand. He had had enough and begged the
doctors to remove it.
In February 2001 Clint Hallam's hand was amputated by Nadey
Hakim, one of the surgeons who had helped attach it in the first
place. The procedure, at a private London clinic, took ninety
minutes. Hallam was relieved to see it gone. Some of the surgeons
who had enjoyed such acclaim only a few years before were angry
that their work had been in vain; that their patient had not persisted
with his medication.
In retrospect, Clint Hallam was probably the wrong person to
receive the world's first hand transplant. If he had done exactly what
he was told – had taken his medication, had followed doctor's
orders – he might still be walking around with a dead man's hand.
Even so, he would have had to cope with the physical symptoms, the
strict drug regime and probably a shorter lifespan as a result of
diabetes or perhaps cancer. Eight years after his transplant, Hallam
was once again fitted with an artificial limb. He claims he has no
regrets about having the transplant; his only regret is being the first.
The case of Clint Hallam illustrates the barriers that have to be
overcome for successful transplantation – whether it is the transplantation
of a hand, finger, kidney or heart. The first barrier is
simply one of technique. It has taken more than a century to
develop the surgery of transplantation. Stitching together blood
vessels is difficult enough, let alone trying to join muscles, tendons
and nerves. But the operation itself is only the start. Next there is
the enormous problem of rejection. The body's immune system will
fight any alien tissue. Even with the latest drugs, rejection is still a
major hurdle for transplant surgeons.
The final problem is more subtle, and is downplayed or ignored
by surgeons at their peril. Any transplantation involves overcoming
a psychological barrier. What is the effect of having a dead man's
hand transplanted on to your arm? It certainly bothered that
woman on the plane. Did Hallam ever think about the motorcyclist
who had died? Before the transplant that hand had been gripping a
motorcycle handle – an essential part of a whole different human
being. What about the psychological effects of a kidney or heart
transplant or even a face?
The surgeons who had operated on Clint Hallam had overcome
the technical problems. Until he stopped taking them, the drugs
had countered his body's physical rejection. But the surgeons had
failed to overcome the final barrier. Consciously or not, it was
Hallam himself who had rejected the hand.
James Spence (and Sons), Soho, London, 1765
James Spence was always very discreet. No one, he assured the
young lady, need ever know that she had visited him. Of course,
nowadays he rarely conducted these procedures himself. He left
most of the day-to-day work to his sons. However, for this fine lady
he would make an exception. She was fearful of going to see anyone
else (there were so many charlatans about these days). Spence had
already established the finest reputation in London for pulling
teeth, and was proud to call himself a dentist, even though
'dentistry' was only just starting to establish itself as a respectable
profession. There was no one better to go to for a tooth transplant.
Spence preferred to use living donors for his tooth transplants.
They were easy to come by and it avoided the repulsion many
people felt at the idea of eating food with teeth from the dead. Mind
you, teeth taken from cadavers were a lot cheaper, and many
dentists did a roaring trade in teeth extracted from the mouths of
soldiers killed on the battlefield.
Nevertheless, today Spence needed teeth from the mouths of
young women. Earlier that morning he had dispatched a servant to
locate suitable donors in the neighbourhood – women who would
be willing to give up their front teeth. They would be handsomely
rewarded (well, it would be handsome to them; the expense would
make only a small dent in Spence's substantial profit margin). By
mid-morning, several young women were queueing in the alley
behind Spence's offices. He planned to take a few teeth, maybe a
couple from each woman, to see which ones produced the best fit.
His patient arrived accompanied by a friend for support.
Spence ushered the women into his consulting room. The patient
sat down on one of the plush, high-backed leather chairs. At first
glance she was something of a beauty and would, he thought, have
no shortage of suitors. But when he took a look at her mouth he
realized it was little wonder she had come to him for help. Her teeth
were in a terrible state. Her mouth stank of decay, with black rotten
stumps emerging from raw, inflamed gums. She was worried about
the pain she was going to experience. Spence reassured her that she
would hardly feel anything; he stopped himself from telling her that
most of the pain would be experienced by the donors.