Fundamentals of Midwifery: A Textbook for Students (64 page)
Read Fundamentals of Midwifery: A Textbook for Students Online
Authors: Louise Lewis

BOOK: Fundamentals of Midwifery: A Textbook for Students
5.8Mb size Format: txt, pdf, ePub
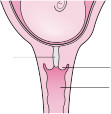
Mucous
plug Cervix
Vagina
Not effaced
Effaced

147
Figure 7.2
Cervix not effaced and cervix effaced. Source: Cruickshank and Shetty 2009, Figure H,
11. Reproduced with permission of Cruickshank and Shetty.presenting part, demonstrates the best indicator of good potential (Figure 7.2 illustrates the not effaced and effaced cervix). Effacement and dilatation of the cervix occurs during the latent phase and despite this being progress, it is not yet regarded as active labour. It can be quite normal for a woman to have an effaced and dilated cervix but not be in active labour. It is only the additional presence of painful and regular uterine contractions that determines the onset of active labour as determined by the National Institute for Health and Clinical Excellence (NICE, 2007).The latent phase has long since been regarded as something the woman is responsible for coping with at home in a normal pregnancy, and does not require admission to a birthing environment. Recommendations are for maternity services to provide one-to-one care once the woman is in established labour (NICE 2007; Hodnett et al. 2013). This suggests that if the woman has a normal pregnancy she does not require midwifery or medical activities or support to assist her during that early phase. There is evidence to suggest that women are more at risk of inter- vention and subsequent assisted birth if admitted in the latent phase of labour, since diagnosing it is so subjective. Becoming more established in labour at home is therefore beneficial (Greulich and Tarrant 2010). However Barnett et al. (2008) reiterate that women have difficulty identifying the onset of labour and seek reassurance from the professionals. Their study concluded that for women, being sent home because they were not in labour only increased their anxiety.If we are aiming to be woman-centred, then maternity service provision needs to consider the individual needs of women and ensure women who are in need during this time, have access to a midwife. As a profession midwifery must not throw the baby out with the bathwater and lose sight of how a midwife must care for the woman rather than her cervix!
Active phase
This active phase of labour is generally regarded as a time where there is no turning back and that labour will progress by further dilatation of the cervix and descent of the fetus through to the impending birth of the baby. Diagnosis of the established and progressive first ‘stage’ of labour is accepted as being from when the cervix of the uterus has dilated (during the latent phase) to four centimetres around the presenting part of the fetus (NICE 2007). Active labour then progresses until the cervix has fully dilated around the presenting part, often termed as being 10 centimetres dilated or ‘fully’, as illustrated in Figure 7.3.Diagnosing dilatation of the cervix and the progress of labour is generally through the con- tinued performance of vaginal examinations, to advise the plan of care, although how often this should be undertaken is open to debate (Downe et al. 2013). Effacement of the cervix and application to the descending part (pressure and stretch) is a most important aspect to consider, indicating good labouring potential, rather than the cervical dilatation measurement alone. A



 148
148
Active phase
This active phase of labour is generally regarded as a time where there is no turning back and that labour will progress by further dilatation of the cervix and descent of the fetus through to the impending birth of the baby. Diagnosis of the established and progressive first ‘stage’ of labour is accepted as being from when the cervix of the uterus has dilated (during the latent phase) to four centimetres around the presenting part of the fetus (NICE 2007). Active labour then progresses until the cervix has fully dilated around the presenting part, often termed as being 10 centimetres dilated or ‘fully’, as illustrated in Figure 7.3.Diagnosing dilatation of the cervix and the progress of labour is generally through the con- tinued performance of vaginal examinations, to advise the plan of care, although how often this should be undertaken is open to debate (Downe et al. 2013). Effacement of the cervix and application to the descending part (pressure and stretch) is a most important aspect to consider, indicating good labouring potential, rather than the cervical dilatation measurement alone. A
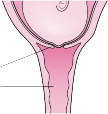
148(b) (c)
Figure 7.3
Progressive dilation of the cervix in the first stage of labour. Source: Cruickshank and Shetty 2009, Figure I, p. 11. Reproduced with permission of Cruickshank and Shetty.
woman could have a cervix dilated to 5 centimetres (cm), but if the presenting part is high and the cervix is not well applied, her contractions may not stimulate the production of oxytocin well. Equally, a woman with a well-effaced cervix at 3 cm dilatation and tightly applied to a low presenting part, has great potential to labour very efficiently, because of the effect the pressure and stretch has on the production of oxytocin (see ‘Optimal hormonal balance’ below). There are many ways of ‘knowing’ that labour is happening and progressing from the woman’s behav- iour (Walsh 2011). The clinical picture will commonly be described from the bio-physical param- eters in relation to the mechanism of labour; Figure 7.9 illustrates how other factors can affect the progress in labour.
Monitoring progress of the active phase of labour
In common practice and recommended by WHO (1994) and NICE (2007) the pictorial record known as the Partogram is used. This tool is used to demonstrate labour progress, recommend- ing the four-hour action line if 1 cm progress per hour is not achieved. However, a systematic review by Lavender et al. (2008) concluded that further evidence is required to determine the efficacy of its use in normal labour. In a randomised controlled trial conducted by Lavender et al. (2006), the evidence suggested that allowing for a slower rate does not necessarily increase caesarean sections and women can be just as satisfied with longer labours. Enkin et al. (2000) recommend 0.5 cm dilatation per hour as progress in primigravida women; this has been endorsed by the NICE (2007) intrapartum guideline.
Partogram use is underpinned by regular vaginal assessment. Recognising landmarks and interpreting the findings of a vaginal examination is a skill that students focus on and causes some anxiety. Vaginal assessment is a skill, which midwives must utilise as efficiently as possible. Midwives may shy away from performing such intimate examinations on occasion, stating it is not necessary if they feel labour is established and progressing. That may be the case in some situations, but midwives must understand the physiology along with safe parameters of progress and wellbeing to determine when such examinations are required. The skill of the midwife lies in knowing when to do and when not to do. Downe et al. (2013) have determined there is widespread use of vaginal examinations without good evidence of its effectiveness.
Therefore, every vaginal examination performed must be justified. Too frequently midwives fail to define position of the baby on vaginal examination or determine that descent through
the pelvis is not occurring. This information is of crucial importance. If the examination is being done – make it count. The fewer examinations the better, but to ensure that is the case, as much information from that examination must be obtained as possible.

Other books
The Demon You Know by Christine Warren
Red Tape by Michele Lynn Seigfried
Blackthorne (The Brotherhood of the Gate Book 1) by Katt Grimm
Love Ties by Em Petrova
A Highland Duchess by Karen Ranney
Luzo: Reign of a Mafia Don by S. W. Frank
Can You Survive the Zombie Apocalypse? by Max Brallier
Joan Hess - Arly Hanks 02 by Mischief In Maggody
The Dead Walk The Earth (Book 4) by Duffy, Luke
First Dance by Bianca Giovanni