i bc27f85be50b71b1 (57 page)
Read i bc27f85be50b71b1 Online
Authors: Unknown

MUSCULOSKELETAL SYSTEM
183
II
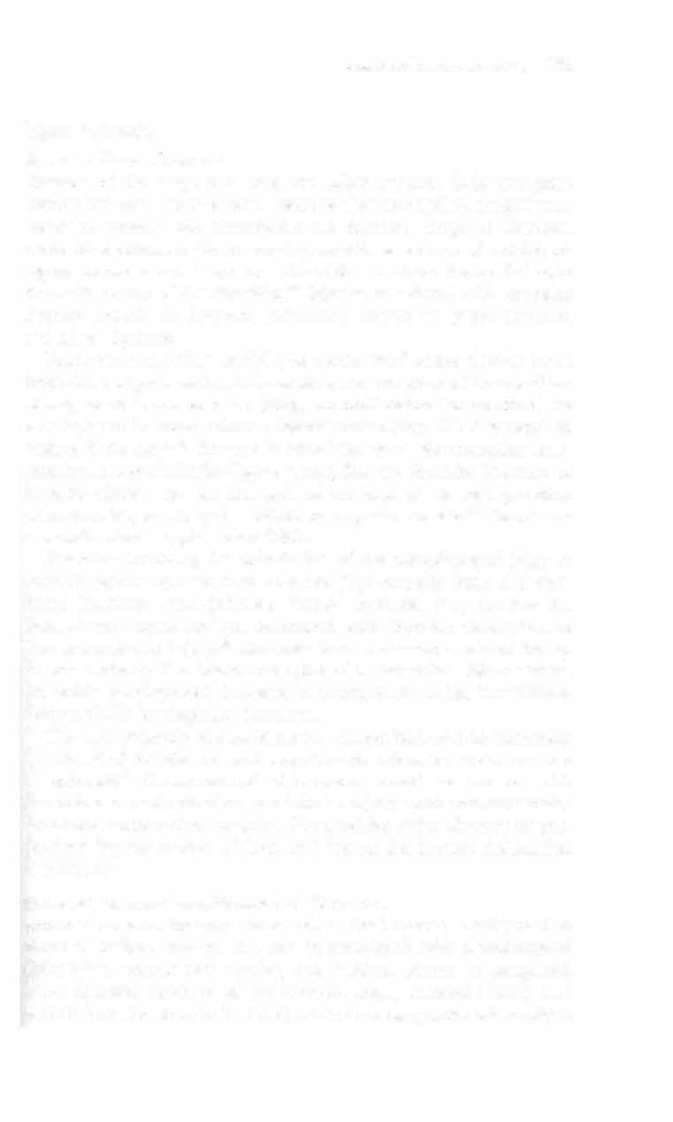
Figure 3-8. Odontoid peg (ractllres. Type I (raetllres o( the upper third o( the
peg. Type II (raetllres at the ;1I/letioll o( the peg with the body o( C2. Type III
(raetllres esselltially o( the body o( C2 at the base o( the peg. (With permission from A Unwin, K Jones /eds/. Emergency Orthopaedics and Trauma.
Boston: Buttertuorth-Heillemamt, 1 995;85.)
respectively. If surgical management is required, it is performed as
soon as the patient is medically stable. Secondary management of spinal fracture may also include the following:
• Examinarion and rrearmenr of associated extremity fracrure or
head or internal injuries


184
A� CARE HAND800K FOR PHYSICAL THERAPISTS
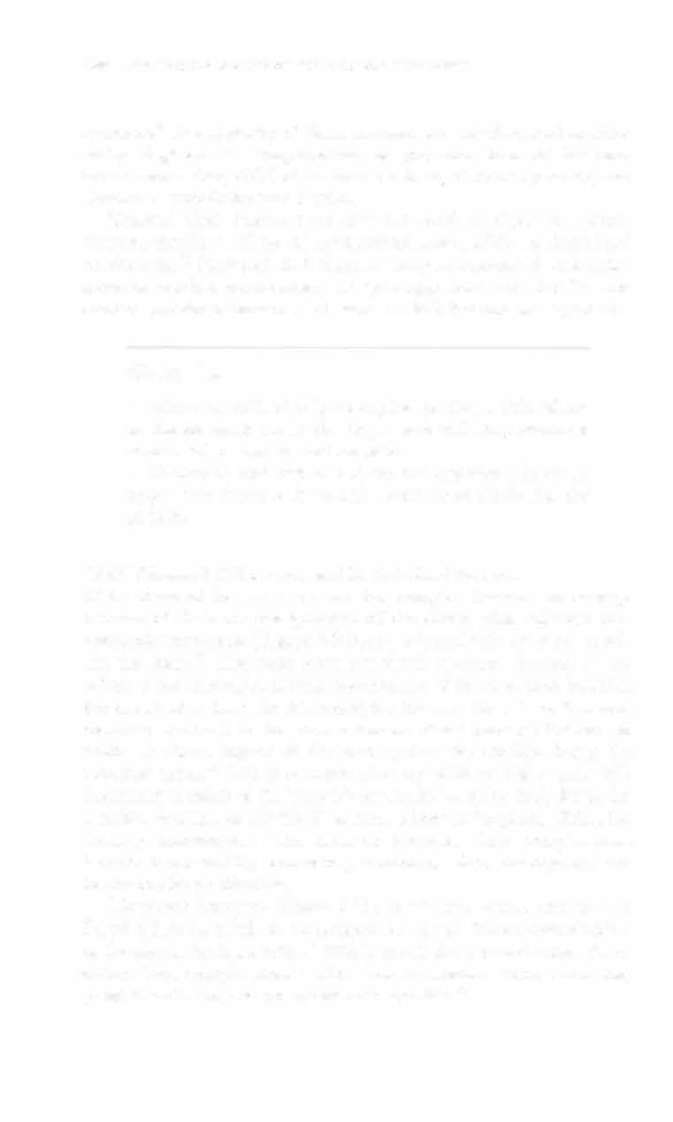
Figure 3-9. Burst fracture. (With permission from A Unwin, K jones /eds/.
Emergency Orthopaedics and Trauma. Boston: Butterworth-Heinemann,
1995;85.)
•
Very frequent (every 15-30 minutes) neurovascular assessment
by nursing
• Close monitoring of airway and brearhing with cervical spine
fractures
Clinical Tip
• Until the cervical, thoracic, and lumbar spines have
been ruled out or "cleared" for fracture, do not remove
temporary immobilization devices (e.g., cervical collar)
until ordered to do so by rhe physician.
• Logroll precautions may exist before spine fracture
clearance. This typically includes bed rest (with the head
of the bed at a 30 degree angle or less) and turning the
patient via logro/! (with rhe head and rorso as a unit).
• Refer to Physical Therapy Intervention after Spinal Surgery for additional tips on mobilizing a patient with back pain or after spinal stabilization.


MUSCULOSKELETAL SYSTE.M 185
Upper Extremity
Shoulder Girdle Fractures
Fracture of the scapula is rare and often requires little treatment
(other than pain management), because the surrounding musculature
serves to protect and immobilize the fracture. Scapular fractures
occur most commonly in 35- to 45-year-olds as a result of a xial loading on an outstretched arm or a direct blow or force from a fall onto the back or top of the shoulder.2• Injuries associated with scapular
fracture include rib fracture, pulmonary contusion, pneumothorax,
and spinal fracture.
Fractures of the distal, middle, or medial third of the clavicle result
from direct impact, such as falls or blows on the point of the shoulder.
Management is conservative (sling immobilization for comfort) for
nondisplaced fractures without ligamentous injury. ORIF is required
acutely if the clavicle fracture is associated with neurovascular compromise, coracoclavicular ligamenr tear, floating shoulder ( fracture of both the clavicle and surgical neck of the scapula), or for separation
of fractute fragments by the deltoid or trapezius muscle.27 Short-term
immobilization is typical after ORJE
Fractures involving the articulation of the glenohumeral joint or
coracoid process are more complicated than scapular body and clavicular fracrures. Intra-articular glenoid fractures may involve the spine of the scapula and are associated with shoulder dislocation or
acromioclavicular injury.28 Coracoid fractures occur at either the tip
or base and may also involve the spine of the scapula.2s Management
for stable nondisplaced fractures is conservative (sling immobilization) or ORIF for displaced fractures.
The vast majority of glenohumeral dislocation occurs anteriorly
as a result of forceful external rotation and extension while the arm
is abducted'> Glenohumeral dislocation should be treated with
immediate closed reduction CO minimize injury to the neurovascular
struc[Ures surrounding the joint. The need for strict dislocation precautions for the patient without risk factors for further dislocation is unlikely.>'
Proximal Humeral alld Humeral Shaft Fractures
Proximal humeral fractures occur when the humerus is subjected to
direct or indirect trauma and can be associated with glenohumeral
dislocation, rotator cuff injuries, and brachial plexus or peripheral
nerve damage. Fracture of the humeral head, ana comic neck, and
lesser tuberosity arc rare; however, fracture of the greater tuberosity is


186
AClfn CARE HANDBOOK FOR PHYSICAL TIIERAPISTS
common.7 The majority of these fractures are nondisplaced or minimally displaced JO Complications of proximal humeral fractures include nonunion, AVN of the humeral head, abnormal posture, and
abnormal scapulothoracic rhythm.
Humeral shaft fractures are also the result of direct or indirect
trauma, usually a fall on an outstretched hand, MVA, or direct load
on the arm.JI Humeral shaft fractures may be associated with radial
nerve or brachial plexus injury. Chapter Appendix Table 3-A.14 summarizes proximal humerus and humeral shaft fracture management.
Clinical Tip
• When the patient is lying supine, placing a thin pillow
or folded sheet under the upper arm will help maintain
neutral alignment and reduce pain.
• Getting in and out of bed on the opposite side of an
upper arm fracture is usually more comfortable for the
patient.
Distal Humeral, Olecranon, and Radial Head Fractures
Distal humeral fractures are rare but complex fractures to manage
because of the bony configuration of the elbow joint, adjacent neurovascular structures (Figure 3-10), and minimal soft tissue surrounding the joint." The mOSt common distal humerus ftacture in the elderly is transcondylar (across the condyles of the olecranon fossa) as