On Killing: The Psychological Cost of Learning to Kill in War and Society (8 page)
Read On Killing: The Psychological Cost of Learning to Kill in War and Society Online
Authors: Dave Grossman
Tags: #Military, #war, #killing

The training methods that increased the firing rate from 15
percent to 90 percent are referred to as "programming" or "conditioning" by some of the veterans I have interviewed, and they do appear to represent a form of classical and operant conditioning (a la Pavlov's dog and B. F. Skinner's rats), which is addressed in detail in the section "Killing in Vietnam." The unpleasantness of this subject, combined with the remarkable success of the army's training programs, and the lack of official recognition might imply that it is classified. But there is no secret master plan responsible for the lack of attention given to this subject. There is instead, in the words of philosopher-psychologist Peter Marin, "a massive 36
KILLING AND THE E X I S T E N C E OF R E S I S T A N C E
unconscious cover-up" in which society hides itself from the true nature of combat. Even among the psychological and psychiatric literature on war, "there is," writes Marin, "a kind of madness at work." He notes, "Repugnance toward killing and the refusal to kill" are referred to as "acute combat reaction." And psychological trauma resulting from "slaughter and atrocity are called 'stress,' as if the clinicians . . . are talking about an executive's overwork."
As a psychologist I believe that Marin is quite correct when he observes, " N o w h e r e in the [psychiatric and psychological] literature is one allowed to glimpse what is actually occurring: the real horror of the war and its effect on those who fought it."
It would be almost impossible to keep something of this nature classified for more than fifty years now, and those in the military w h o do understand — the Marshalls and the Maters — are crying out their messages, but no one wants to hear their truths.
N o , it is not a military conspiracy. There is, indeed, a cover-up and a "conspiracy of silence," but it is a cultural conspiracy of forgetfulness, distortion, and lies that has been going on for thousands of years. And just as we have begun to wipe away the cultural conspiracy of guilt and silence concerning sex, we
must
n o w wipe away this similar conspiracy that obscures the very nature of war.
Chapter Four
The Nature and Source of the Resistance
Where does this resistance to killing one's fellow man come from?
Is it learned, instinctive, rational, environmental, hereditary, cultural, or social? Or some combination thereof?
One of Freud's most valuable insights involves the existence of the life instinct (Eros) and the death instinct (Thanatos). Freud believed that within each individual there is a constant struggle between the superego (the conscience) and the id (that dark, lurk-ing mass of destructive and animal urges residing within each of us), and that the struggle is mediated by the ego (the self). One wit once referred to this situation as "a struggle in a locked, dark basement; between a homicidal sex-crazed monkey and a puritanical old maid; being mediated by a timid accountant."
In battle we see the id, the ego, the superego, Thanatos, and Eros in turmoil within each soldier. The id wields the Thanatos like a club and screams at the ego to kill. The superego appears to have been neutralized, for authority and society say that now it is good to do what has always been bad. Yet something stops the soldier from killing. What? Could it be that Eros, the life force, is much stronger than ever before understood?
Much has been made of the obvious existence and manifestation of Thanatos in war, but what if there is within most men a stronger drive than Thanatos? What if there is within each person a force 38 KILLING AND THE E X I S T E N C E OF R E S I S T A N C E
that understands at some gut level that all humanity is inextricably interdependent and that to harm any part is to harm the whole?
T h e R o m a n emperor Marcus Aurelius understood this force even as he fought desperate battles against the barbarians w h o would ultimately destroy R o m e . "Every individual dispensation,"
wrote Marcus Aurelius, more than a millennia and a half ago, "is one of the causes of the prosperity, success, and even survival of That which administers the universe. To break off any particle, no matter how small, from the continuous concatenation —
whether of causes or of any other elements — is to injure the whole."
Holmes records another veteran who, almost two millennia after Marcus Aurelius, grasped the same concept when he observed that some of the marines he was with in Vietnam reached a point of reflection after battle in which they "came to see the young Vietnamese they had killed as allies in a bigger war of individual existence, as young men with w h o m they were united throughout their lives against the impersonal 'thems' of the world." Holmes then makes a timeless and powerful perception about the psyche of the American soldier when he notes that "in killing the grunts of N o r t h Vietnam, the grunts of America had killed a part of themselves."
Perhaps this is why we avoid this truth. Perhaps to truly understand the magnitude of the resistance to killing is also to understand the magnitude of man's inhumanity to man. Glenn Gray, driven by his own personal guilt and anguish resulting from his World War II experiences, cries out with the pain of every self-aware soldier w h o has thought this matter through: " I , too, belong to this species. I am ashamed not only of my o w n deeds, not only of my nation's deeds, but of human deeds as well. I am ashamed to be a man.
" T h i s , " says Gray, "is the culmination of a passionate logic which begins in warfare with the questioning of some act the soldier has been ordered to perform contrary to his conscience."
If this process continues, then "consciousness of failure to act in response to conscience can lead to the greatest revulsion, not only for oneself, but for the human species."
T H E N A T U R E A N D S O U R C E OF THE R E S I S T A N C E 39
We may never understand the nature of this force in man that causes him to strongly resist killing his fellow man, but we can give praise for it to whatever force we hold responsible for our existence. And although military leaders responsible for winning a war may be distressed by it, as a race we can view it with pride.
There can be no doubt that this resistance to killing one's fellow man is there and that it exists as a result of a powerful combination of instinctive, rational, environmental, hereditary, cultural, and social factors. It is there, it is strong, and it gives us cause to believe that there may just be hope for mankind after all.
S E C T I O N I I
Killing and Combat Trauma:
The Role of Killing in Psychiatric Casualties
Nations customarily measure the "costs of war" in dollars, lost production, or the number of soldiers killed or wounded. Rarely do military establishments attempt to measure the costs of war in terms of individual human suffering. Psychiatric breakdown remains one of the most costly items of war when expressed in human terms.
— Richard Gabriel
No More Heroes
Chapter One
The Nature of Psychiatric Casualties:
The Psychological Price of War
Richard Gabriel tells us that "in every war in which American soldiers have fought in this century, the chances of becoming a psychiatric casualty — of being debilitated for some period of time as a consequence of the stresses of military life — were greater than the chances of being killed by enemy fire."
During World War II more than 800,000 men were classified 4-F (unfit for military service) due to psychiatric reasons. Despite this effort to weed out those mentally and emotionally unfit for combat, America's armed forces lost an additional 504,000 men from the fighting effort because of psychiatric collapse — enough to man fifty divisions! At one point in World War II, psychiatric casualties were being discharged from the U.S. Army faster than new recruits were being drafted in.
In the brief 1973 Arab-Israeli War, almost a third of all Israeli casualties were due to psychiatric causes, and the same seems to have been true among the opposing Egyptian forces. In the 1982
incursion into Lebanon, Israeli psychiatric casualties were twice as high as the number of dead.
Swank and Marchand's much-cited World War II study determined that after sixty days of
continuous
combat, 98 percent of all
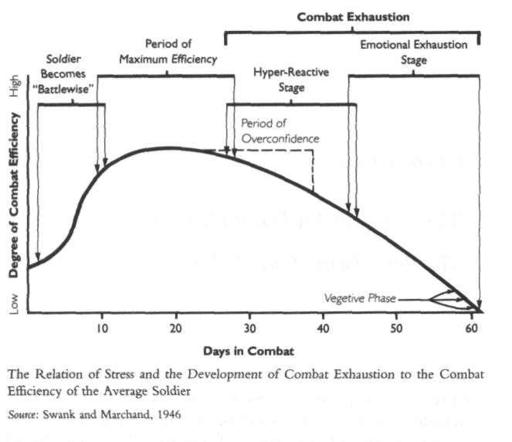
44
KILLING AND C O M B A T T R A U M A
surviving soldiers will have become psychiatric casualties of one kind or another. Swank and Marchand also found a common trait among the 2 percent who are able to endure sustained combat: a predisposition toward "aggressive psychopathic personalities."
The British in World War I believed that their soldiers were good for several hundred days before inevitably becoming a psychiatric casualty. But this was only made possible by the British policy of rotating men out of combat for four days of rest after approximately twelve days of combat, as opposed to America's World War II policy of leaving soldiers in combat for up to eighty days at a stretch.
It is interesting to note that spending
months of continuous
exposure to the stresses of combat is a phenomenon found only on the battlefields of this century. Even the years-long sieges of previous THE NATURE OF PSYCHIATRIC CASUALTIES
45
centuries provided ample respites from combat, largely due to limitations of artillery and tactics. The actual times of personal risk were seldom more than a few hours in duration. Some psychiatric casualties have always been associated with war, but it is only in this century that our physical and logistical capability to sustain combat has completely outstripped our psychological capacity to endure it.
The Manifestations of Psychiatric Casualties
In his book
No More Heroes
Richard Gabriel examines the many historical symptoms and manifestations of psychiatric casualties.1
Among these are fatigue cases, confusional states, conversion hysteria, anxiety states, obsessional and compulsive states, and character disorders.
Fatigue Cases
This state of physical and mental exhaustion is one of the earliest symptoms. Increasingly unsociable and overly irritable, the soldier loses interest in all activities with comrades and seeks to avoid any responsibility or activity involving physical or mental effort. He becomes prone to crying fits or fits of extreme anxiety or terror.
There will also be such somatic symptoms as hypersensitivity to sound, increased sweating, and palpitations. Such fatigue cases set the stage for further and more complete collapse. If the soldier is forced to remain in combat, such collapse becomes inevitable; the only real cure is evacuation and rest.
Confusional States
Fatigue can quickly shift into the psychotic dissociation from reality that marks confusional states. Usually, the soldier no longer knows who he is or where he is. Unable to deal with his environment, he has mentally removed himself from it. Symptoms include delirium, psychotic dissociation, and manic-depressive mood swings. One often noted response is Ganzer syndrome, in which the soldier will begin to make jokes, act silly, and otherwise try to ward off the horror with humor and the ridiculous.
46
KILLING AND C O M B A T T R A U M A
T h e degree of affliction in confusional states can range from the merely neurotic to the overtly psychotic. T h e sense of humor exhibited in the movie and television series
M*A*S*H is
an excellent example of individuals mildly afflicted with Ganzer syndrome.
And this personal narrative provides a look at a man severely afflicted with Ganzer syndrome:
"Get that thing out of my face, Hunter, or I'll feed it to you with hot sauce."
"C'mon, Sarge, don't you want to shake hands with 'Herbert'?"
"Hunter, you're f ed up. Anybody who'd bring back a gook arm is sick. Anybody who'd bring one in the tent is begging for extra guard. You don't know where that thing's been. QUIT
PICKING Y O U R NOSE WITH IT! OUT, HUNTER! OUT!"
"Aw, Sarge, 'Herbert' just wants to make friends. He's lonely without his old friends, 'Mr. Foot' and 'Mr. Ballbag.' "
"Double guard tonight, Hunter, and all week. Goodbye, sicko.
Enjoy your guard."
"Say good night to 'Herbert,' everyone."
"OUT! OUT!"
Black humor of course. Hard laughs for the hard guys. After a time, nothing was sacred. If Mom could only see what her little boy was playing with now.
Or what they were paying him to do.
— W. Norris
"Rhodesia Fireforce Commandos"
Conversion Hysteria
Conversion hysteria can occur traumatically during combat or post-traumatically, years later. Conversion hysteria can manifest itself as an inability to know where one is or to function at all, often accompanied by aimless wandering around the battlefield with complete disregard for evident dangers. U p o n occasion the soldier becomes amnesiatic, blocking out large parts of his memory.
Often, hysteria degenerates into convulsive attacks in which the soldier rolls into the fetal position and begins to shake violently.
THE NATURE OF PSYCHIATRIC CASUALTIES 47
Gabriel notes that during both world wars cases of contractive paralysis of the arm were quite common, and usually the arm used to pull the trigger was the one that became paralyzed. A soldier may become hysterical after being knocked out by a concussion, after receiving a minor nondebilitating wound, or after experiencing a near miss. Hysteria can also show up after a wounded soldier has been evacuated to a hospital or rear area. Once he is there, hysteria can begin to emerge, most often as a defense against returning to fight. Whatever the physical manifestation, it is always the mind that produces the symptoms, in order to escape or avoid the horror of combat.
Anxiety States
These states are characterized by feelings of total weariness and tenseness that cannot be relieved by sleep or rest, degenerating into an inability to concentrate. When he can sleep, the soldier is often awakened by terrible nightmares. Ultimately the soldier becomes obsessed with death and the fear that he will fail or that the men in his unit will discover that he is a coward. Generalized anxiety can easily slip into complete hysteria. Frequently anxiety is accompanied by shortness of breath, weakness, pain, blurred vision, giddiness, vasomotor abnormalities, and fainting.
Another reaction, which is commonly seen in Vietnam veterans suffering post-traumatic stress disorder (PTSD), years after combat, is emotional hypertension, in which the soldier's blood pressure rises dramatically with all the accompanying symptoms of sweating, nervousness, and so on.2
Obsessional and Compulsive States
These states are similar to conversion hysteria, except that here the soldier realizes the morbid nature of his symptoms and that his fears are at their root. Even so, his tremors, palpitations, stam-mers, tics, and so on cannot be controlled. Eventually the soldier is likely to take refuge in some type of hysterical reaction that allows him to escape psychic responsibility for his physical symptoms.
48 KILLING AND COMBAT TRAUMA
Character Disorders
Character disorders include obsessional traits in which the soldier becomes fixated on certain actions or things; paranoid trends accompanied by irascibility, depression, and anxiety, often taking on the tone of threats to his safety; schizoid trends leading to hypersensitivity and isolation; epileptoid character reactions accompanied by periodic rages; the development of extreme dramatic religiosity; and finally degeneration into a psychotic personality.
What has happened to the soldier is an altering of his fundamental personality.
These are only some of the possible symptoms of psychiatric casualties in war. Gabriel notes that "The mind has shown itself infinitely capable of bringing about any number of combinations of symptoms and then, to make matters worse, burying them deep in the soldier's psyche so that even the overt manifestations become symptoms of deeper symptoms of even deeper underlying causes."
The key understanding to take away from this litany of mental illness is that within a few months of sustained combat
some symptoms of stress
will develop in almost all participating soldiers.
Treating the Mentally Maimed
Treatment for these many manifestations of combat stress involves simply removing the soldier from the combat environment. Until the post-Vietnam era, when hundreds of thousands of PTSD cases appeared, this was the only treatment believed necessary to permit the soldier to return to a normal life. But the problem is that the military does not want to simply return the psychiatric casualty to normal life, it wants to return him to combat! And he is understandably reluctant to go.
The evacuation syndrome is the paradox of combat psychiatry.
A nation must care for its psychiatric casualties, since they are of no value on the battlefield — indeed, their presence in combat can have a negative impact on the morale of other soldiers — and they can still be used again as valuable seasoned replacements once they've recovered from combat stress. But if soldiers begin to realize that insane soldiers are being evacuated, the number of THE NATURE OF PSYCHIATRIC CASUALTIES
49
psychiatric casualties will increase dramatically. An obvious solution to this problem is to rotate troops out of battle for periodic rest and recuperation — this is standard policy in most Western armies — but this is not always possible in combat.
Proximity — or forward treatment — and expectancy are the principles developed to overcome the paradox of evacuation syndrome. These concepts, which have proved themselves quite effective since World War I, involve (1) treatment of the psychiatric casualty as far forward on the battlefield as possible — that is, in the closest possible
proximity
to the battlefield, often still inside enemy artillery range — and (2) constant communication to the casualty by leadership and medical personnel of their
expectancy
that he will be rejoining his comrades in the front line as soon as possible. These two factors permit the psychiatric casualty to get the much-needed rest that is the only current cure for his problem, while not giving a message to still-healthy comrades that psychiatric casualty is a ticket off of the battlefield.
Limited chemical treatments have been used in recent years to assist in the recovery process. According to Watson, "the so-called truth drugs have also been used near the front line to 'abreact'
soldiers who are shell-shocked." Such drugs have reportedly been used with some success by the Israelis to induce psychiatric casualties to "talk through the circumstances leading to their reaction, an activity which appears to prevent their fears being 'bottled up'
and so causing some other, long-term syndrome."
But the use of chemicals in combat may not be quite so benign in the future. Gabriel, a retired intelligence officer and consultant to both the House and Senate Armed Services Committees, provides a chilling note on the future of the treatment and prevention of combat psychiatric casualties. He believes that the armed forces of both the West and the East are searching for a chemical answer to this problem. Gabriel warns that the perfection of a "nondepleting neurotrop" to be given to soldiers prior to battle would result in
"armies of sociopaths."
Gabriel concludes from his research that "one can but marvel at the inventiveness of the human psyche in its efforts to escape its surrounding horror." Similarly, we must marvel at the 50 KILLING AND COMBAT TRAUMA
inventiveness of modern armies and nations in their efforts to ensure that they get full value from their soldiers. And we cannot help but come away with an image of war as one of the most horrifying and traumatic acts a human being can participate in. War is an environment that will psychologically debilitate 98 percent of all who participate in it for any length of time. And the 2 percent who are not driven insane by war appear to have already been insane — aggressive psychopaths — before coming to the battlefield.