Resident Readiness General Surgery (28 page)
Read Resident Readiness General Surgery Online
Authors: Debra Klamen,Brian George,Alden Harken,Debra Darosa
Tags: #Medical, #Surgery, #General, #Test Preparation & Review

Untreated and severe Type B and C symptoms may lead to complicated withdrawal. It may be difficult to separate these symptom clusters entirely as they represent dynamic neurotransmitter systems that are interrelated and, importantly, may become dysfunctional from other medical/surgical etiologies.
COMPREHENSION QUESTIONS
1.
Which of the following describes symptoms of complicated alcohol withdrawal?
A. Slurred speech, ataxia, and nystagmus
B. Agitation, diaphoresis, and presence of visual hallucinations
C. Anxiety, restlessness, mild tremor, and nausea
D. Lacrimation, diarrhea, diaphoresis, and myalgia
2.
Which of the following describes symptoms of early alcohol withdrawal?
A. Breath smelling of alcohol, slurred speech, and ataxia
B. Agitation, hypertension, and tactile hallucinations
C. Tremors, mild anxiety, and diaphoresis
D. Lacrimation, diarrhea, diaphoresis, and myalgias
3.
Of the following, which is the highest-risk patient for alcohol withdrawal delirium?
A. A 20-year-old man, (+) BAL, elevated AST:ALT ratio, normal MCV, consumes 6 beers/day for the last month
B. A 40-year-old woman, (-) BAL, drinks 1 to 2 drinks/week, no history of DUIs
C. A 50-year-old man, (+) BAL, elevated AST:ALT ratio, elevated MCV, consumes 6 beers/day for the last month
D. A 55-year-old man, (+) BAL, normal MCV, normal liver function tests
4.
Which of the following is a long-acting benzodiazepine?
A. Chlordiazepoxide
B. Oxazepam
C. Lorazepam
D. Midazolam
Answers
1.
B
. Seizures and hallucinations, along with autonomic dysfunction and the presence of delirium, are signs and symptoms of complicated alcohol withdrawal. Choice A describes benzodiazepine intoxication. Choice C describes uncomplicated alcohol withdrawal. Choice D represents symptoms of opioid withdrawal.
2.
C
. Tremulousness, anxiety, headache, palpitations, anorexia, nausea, and GI upset are all signs and symptoms of uncomplicated alcohol withdrawal.
3.
C
. While both A and C carry the highest risk of the scenarios presented, the patient in answer C is greater than 35 years old (increased risk factor) versus the patient in A, in which his younger age should provide some protection. In addition, the patient in C has an elevated MCV in the presence of an elevated AST:ALT ratio, likely corresponding to a longer and heavier drinking history.
4.
A
. Chlordiazepoxide has a half-life of 30 to 100 hours. Choices B and C are all intermediate-acting benzodiazepines, and D is a short-acting benzodiazepine.
 A 50-year-old Man Presenting With Extensive Burns
A 50-year-old Man Presenting With Extensive Burns
Jeremy Goverman, MD, FACS and Shawn P. Fagan, MD, FACS
A 50-year-old, 75-kg, male is brought into the emergency department by EMS. He was found ambulating at the scene of a house fire approximately 2 hours prior. He is noted to have circumferential third-degree burns to his entire right and left upper extremities as well as his entire head and neck. In the emergency department he is alert and oriented, and complains of a dry mouth.
1.
What is the first step in assessing this patient?
2.
How large is this patient’s burn?
3.
According to the Parkland formula, how much fluid will this patient need during the first 8 hours? Next 16 hours? What is the initial intravenous fluid rate?
4.
Should this patient be transferred to an American Burn Association–verified Burn Center?
5.
Why is it important to know if a burn is circumferential? What procedure would you perform?
BURNS
Answers
1.
As with every trauma, begin with ATLS protocol and assessment of ABCs. In this case the patient will require intubation for airway protection. Given the size (>20%) and location of the burn, the patient will require large-volume resuscitation and will likely develop significant facial and airway edema. Elective intubation prior to the development of airway edema is common practice for larger burns.
2.
The rule of 9’s allows for a simplified approach to calculate total body surface area (TBSA) for a burn (
Figure 21-1
). The Lund and Browder method (which utilizes a chart) is commonly used for estimation of burn size in children.
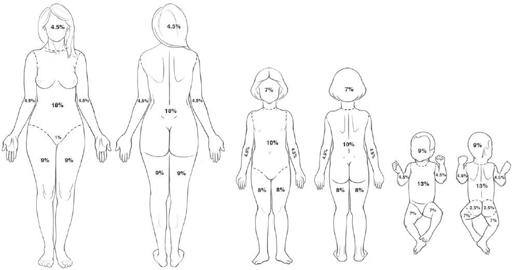
Figure 21-1.
The rule of 9’s. (Reproduced with permission from Kaufman MS, Stead LG, Stead SM, et al.
First Aid for the Surgery Clerkship
. 2nd ed. New York: McGraw-Hill; 2009:299 [Figure 18-1].)
In the case above, each upper extremity is 9, head is 9, neck is 1 = 28% TBSA.
3.
The Parkland formula is a formula used for the initial fluid resuscitation of a burn patient with >20% TBSA. It estimates the overall fluid total as 4 mL × % TBSA × weight (kg). Half of this volume is to be administered in the first 8 hours post burn, while the second half of this volume is to be administered over the next 16 hours.
The Parkland formula should only serve as a guide to resuscitation. Global (ie, lactate, base deficit, pH) and regional (ie, urine output, mental status) parameters of perfusion should be followed and trended in order to fine-tune the resuscitation volumes. Typically crystalloid is used for the first 8 hours and varying quantities of colloid (ie, albumin) are added in according to patient needs and surgeon preference. As resuscitation volumes approach and exceed 6 cm
3
/% TBSA/kg, the incidence of compartment syndromes and intra-abdominal hypertension increases. In such cases, the addition of colloid may allow for slightly less overall fluid administration.
In this case 4 mL × 28% third-degree burn × 75 kg = 8400 cm
3
. This is the total fluid to be given over 24 hours (4200 cm
3
/first 8 hours, 4200 cm
3
/next 16 hours). Since the patient presented 2 hours post injury, the first 4200 cm
3
should be given over 6 hours. IVF rates would be 700 cm
3
/h (first 6 hours), and 262.5 cm
3
/h (second 16 hours).