Secondary Schizophrenia (123 page)
Read Secondary Schizophrenia Online
Authors: Perminder S. Sachdev

250. Gu S., Pakstis A. J., Li H.,
et al.
populations. Eur J Hum Genet,
of association in genome scans.
Significant variation in haplotype
2007.
15
:302–12.
308
Section 3
Organic syndromes of schizophrenia: genetic disorders related to SLP
24Velocardiofacialsyndrome(chromosome
22q11.2 deletion syndrome) as a model of
schizophrenia
Vandana Shashi and Margaret N. Berry
Facts box
developmental theory suggests that neurocognitive
r
and neuroanatomical abnormalities often precede the
Velocardiofacial syndrome (VCFS), caused
development of overt psychosis. The delineation of
by a heterozygous deletion of chromosome
the progression of these often subclinical neurocogni-22q11.2, is associated with congenital
tive and morphological brain anomalies provides an
anomalies, medical complications, and
opportunity to identify at-risk individuals, improve
cognitive impairment.
the understanding of the pathogenesis of this com-r
VCFS is associated with an extraordinarily
plex disorder, and ultimately hasten the development
high risk (30%–40%) of major psychiatric
of prophylactic interventions.
illnesses, in late adolescence and early
Numerous epidemiological and genetic linkage
adulthood, mainly schizophrenia (25%–30%)
studies have provided incontrovertible evidence that
but also schizotypy, bipolar illness, and major
genetic factors are important in the predisposition to
depression.
schizophrenia spectrum disorders
[3, 4, 5]
, with the
r
It has been found that 1%–2% of individuals
heritability estimated to be 60%–90%
[6].
However,
with schizophrenia in the general population
gene identification has largely been unsuccessful, due
have a 22q11.2 deletion, whereas 5% of
to the complex nature of the inheritance of the genes
patients with childhood-onset schizophrenia
and the probability that multiple genes of individual
will have VCFS upon testing.
modest effect are involved. Identification of predispos-r
The early neurocognitive manifestations in
ing genetic markers would provide a model that would
VCFS are similar to those that would be
enable the prospective study of the factors contributing
expected to occur on the pathway to
to psychosis in a high-risk group of individuals.
schizophrenia.
Velocardiofacial syndrome (VCFS), caused by a
r
heterozygous deletion of chromosome 22q11.2, is
The brain structural abnormalities in VCFS
associated with congenital anomalies, medical com-have many parallels with those seen in
plications, and cognitive impairment. Since the early
schizophrenia.
r
1990s, retrospective studies have reported a markedly
In individuals with VCFS, there is
high incidence (
∼
40%) of schizophrenia and mood
controversy about the relationship between
psychoses in late adolescence and adulthood in ind-the COMT genotype, the cognitive deficits,
ividuals with the deletion
[7, 8, 9, 10].
The risk
and schizophrenia. There are other genes of
of schizophrenia spectrum disorders in VCFS ap-interest in the deletion region that may be of
proaches that of a monozygotic twin of a patient with
relevance to schizophrenia.
r
schizophrenia, or that of an individual with two par-Mouse models of VCFS have proven to be of
ents with schizophrenia. These observations provide the
limited value in understanding the
strongest known link between psychosis and an identi-mechanisms involved in psychosis.
fied genetic condition. In addition, because the signs,
symptoms, and response to treatment of schizophrenia in this disorder are thought to be no different
to that in the general population, it has been sug-In recent years, schizophrenia has been viewed as
gested that VCFS represents an ideal model for the
309
a neurodevelopmental disorder
[1, 2].
This neuro-study of schizophrenia
[11].
This chapter delineates the
Organic Syndromes of Schizophrenia – Section 3
Table 24.1
Features that should warrant testing for VCFS in patients with schizophrenia (modified from [15])
Psychiatric
Dev/psychological
Medical history
Family history
Physical examination
Mental retardation
Developmental delay
Conotruncal heart anomalies
∗
VCFS in first
Low anterior hairline
degree relative
∗
Borderline IQ
Hypernasal speech
∗
Hypoparathyroidism
∗
Conotruncal Heart
Hooded eyelids
Anomalies
∗
Depression
Learning disability
VPI, submucous cleft
∗
Surgery for Palate
External ear anomalies
∗
Abnormalities
Anxiety disorder
T cell immune deficiency
∗
Bulbous nasal tip, wide
middle part of nose
∗
Feeding difficulty with
Asymmetric crying facies
∗
nasopharyngeal reflux
∗
Renal anomalies
∗
(including
Long slender fingers
missing kidney)
Autoimmune disease–vitiligo,
Hypospadius, polydactyly
Graves Disease, juvenile
imperforate anus long,
rheumatoid arthritis, idiopathic
slender fingers
thrombocytopenic purpura
∗
Indicates that the presence of this feature alone is sufficient to consider FISH testing. Otherwise, the presence of two or more features
should prompt a genetics referral and/or FISH testing.
Common heart anomalies seen in VCFS include tetralogy of fallot, interrupted aortic arch, truncus arteriosus, ventricular septal defect, atrial
septal defect and a vascular ring.
psychological and psychiatric findings, brain mor-with the condition and thus a high index of suspicion
phometric abnormalities, and the genetic studies that
needs to be maintained. A history of a congeni-underscore the importance of VCFS in understanding
tal abnormality or a host of medical and develop-the neurodevelopmental trajectory of schizophrenia.
mental problems should prompt referral to a clinical geneticist. The clinical diagnosis is made typically
during one of the following time periods: (i) prena-
Velocardiofacial syndrome
tally, when a conotruncal heart anomaly is detected
Deletion of chromosome 22 at band q11.2 result-with or without other structural organ abnormalities,
ing in VCFS is the most common chromosome
(ii) in infancy, due to conotruncal heart abnormali-microdeletion syndrome in human beings, occurring
ties, hypocalcemia, immune deficiency, other medi-with an incidence of 1/2000 to 1/6000 births
[12,
cal problems, and developmental delays, (iii) during
13, 14].
Also known as chromosome 22q11.2 dele-the childhood years, due to speech difficulties related
tion syndrome, DiGeorge syndrome, or Cayler car-to velopharyngeal insufficiency (often needing surgi-diofacial syndrome, it is commonly associated with
cal repair) and cognitive problems, (iv) in adulthood,
learning disabilities (80%–100%), congenital heart
due to the occurrence of major psychiatric illnesses
disease (70%), palatal abnormalities (70%), immune
and/or having a child with the condition. At all ages,
deficiency (70%), hypoparathyroidism (60%), feed-the typical facial features can be evident, including a
ing problems (30%), and characteristic facial features.
low anterior hairline, hooded upper eyelids, widening
Mental retardation is seen in 50% of affected individu-of the middle part of the nose or a bulbous nasal tip,
als. Although more than 180 manifestations have been
ear anomalies, and a small chin
(Figure 24.1).
How-reported, illustrating the extent of the clinical vari-ever, as with all the other features in the condition, the
ability of the condition, the diagnosis should be sus-facial abnormalities may be variable and can be subpected when one or more of the more common fea-tle or not discernible
(Figure 24.2)
and thus the diag-tures are present in the individual patient
(Table 24.1).
nosis may be missed, unless a high index of suspicion
It is to be emphasized that, undoubtedly, many indi-is maintained. The clinical suspicion is confirmed by
viduals with VCFS, being evaluated and treated by
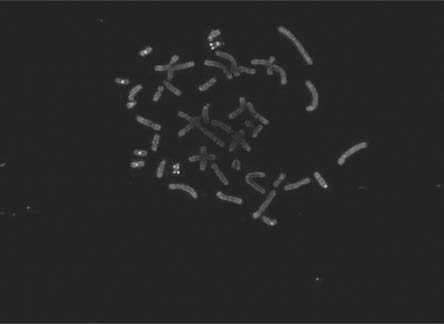
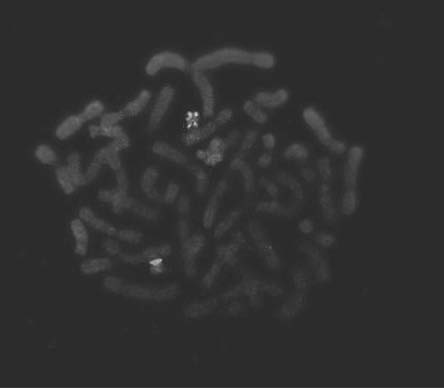
the detection of the microdeletion by fluorescence in-
310
mental health professionals, have not been diagnosed
situ hybridization (FISH) analysis
(Figure 24.3).
Most

Chapter 24 – Velocardiofacial syndrome
(A)
(B)
Figure 24.1
Ten year-old boy with VCFS, demonstrating hooded
upper eyelids, widened middle part of the nose, and ear
abnormalities.