Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (1023 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
4.6Mb size Format: txt, pdf, ePub
IGF-I and IGFBP-3 reference ranges are highly age dependent, and results must always be interpreted within the context of the patient’s age.
INSULIN-LIKE GROWTH FACTOR-I (IGF-I)
Definition
Normal range:
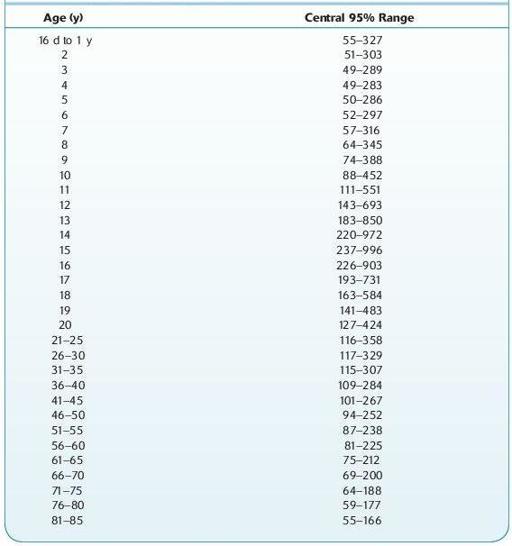
see Table 16.50; 0–7 days: <26 ng/mL; 8–15 days: <41 ng/mL.
TABLE 16–50. Normal Range of IGF-I
Other books
A Little History of Literature by John Sutherland
Reluctant Date by Sheila Claydon
Reefs and Shoals by Lambdin, Dewey
Nicademus: The Wild Ones by Sienna Mynx
Forbidden: Ultimate Stepbrother Collection by Anna Hard
Lady Ann's Excellent Adventure (A Regency Short Story) by Hern, Candice
Everlastin' Book 1 by Mickee Madden
War From The Clouds by Nick Carter
The Borgias by Christopher Hibbert
The Red Chamber by Pauline A. Chen