Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (136 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
12.43Mb size Format: txt, pdf, ePub
Structural (e.g., diaphragmatic hernia, jejunal atresia, volvulus, intestinal malrotation) Peritonitis caused by GI tract perforation, congenital infection (e.g., syphilis, TORCH [
t
oxoplasmosis,
o
ther agents,
r
ubella,
C
MV, and
h
erpes simplex], hepatitis), meconium peritonitis
M1
gangliosidosis type I, I-cell disease, β-glucuronidase deficiency)
Immune (maternal antibodies reacting to fetal antigens [e.g., Rh, C, E, Kell])
PERITONITIS, ACUTE
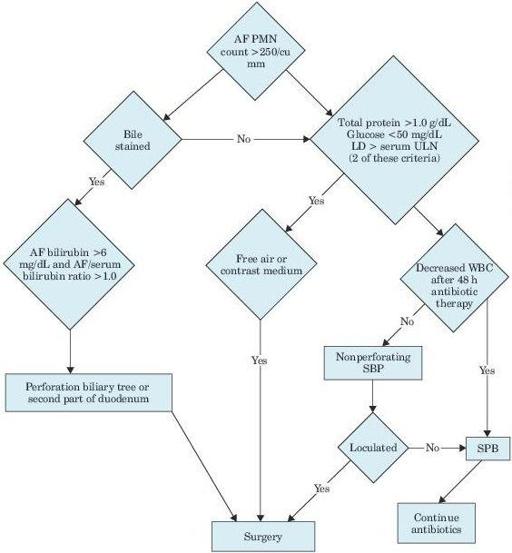
Figure 5–3
Algorithm for differentiating secondary from spontaneous bacterial peritonitis. AF, ascitic fluid; PMN, polymorphonuclear leukocytes; LD, lactate dehydrogenase; ULN, upper limit of normal; WBC, white blood cell; SBP, spontaneous bacterial peritonitis.
Other books
Judgment by Sean Platt and Johnny B. Truant
The Aloha Quilt by Jennifer Chiaverini
The Adventures of Nicholas by Helen Siiteri
The Heir of Olympus and the Forest Realm by Zachary Howe
The Colossal Camera Calamity by Anonymous
The Jovian Run: Sol Space Book One by James Wilks
Targets of Deception by Jeffrey Stephens
Harlequin Intrigue June 2015 - Box Set 1 of 2: To Honor and To Protect\Cornered\Untraceable by Debra & Regan Webb & Black
Deadly Echoes by Philip Donlay
The Silver Fox and the Red-Hot Dove by Deborah Smith