Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (171 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
12.98Mb size Format: txt, pdf, ePub
A diagnosis of intrahepatic cholestasis made by clinical assessment and supported by negative findings from ultrasound or CT scan offers 95% specificity. In a patient in whom extrahepatic obstruction is not strongly suspected, no further investigation of the extrahepatic biliary tree is indicated.
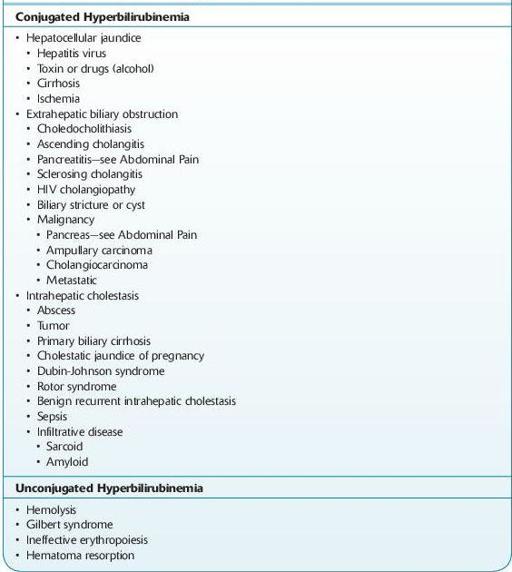
TABLE 5–6. Differential Diagnosis of Jaundice
HYPERBILIRUBINEMIA
UNCONJUGATED HYPERBILIRUBINEMIA
Causes
Increased destruction of RBCs
Infection (viral, bacterial, and protozoal)
Other books
The Killing 3 by Hewson, David
The Protege by Kailin Gow
INFECTED (Click Your Poison) by Schannep, James
The Last Days by Laurent Seksik
Adventures of a Middle School Zombie by Scott Craven
The Turkish Baths (When Straight Guys Go Gay) by E.M. Bridger
Absolute Beginners (Absolute #1) by S.J. Hooks
White People by Allan Gurganus
Viator (The Viator Chronicles Book 1) by Ralston-Brooks, Jane
Succulence (Succulent Trilogy #1) by Lauren Lashley