Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (198 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
10.13Mb size Format: txt, pdf, ePub
Drugs (e.g., estrogens, anabolic steroids)—most common cause (Table
5-13
)
Autosomal recessive condition; attacks begin after age 8, last weeks to months, complete resolution between episodes, may recur after months or years; exacerbated by estrogens
TABLE 5–13. Comparison of Various Types of Cholestatic Disease
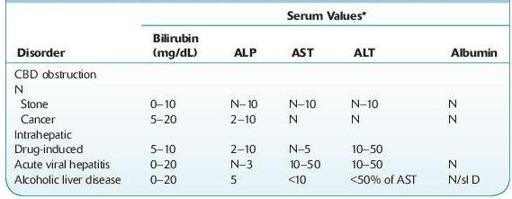
CBD, common bile duct; N, normal; sl D, slightly decreased.
*Serum value, times normal.
Laboratory Findings
Core laboratory
: Increased serum ALP, but GGT is usually normal. Serum direct bilirubin may be normal or ≤10 mg/dL. Transaminase usually <100 U.
Histology
: Liver biopsy shows centrolobular cholestasis without inflammation, bile pigment in hepatocytes and canaliculi; little or no fibrosis.
CIRRHOSIS, PRIMARY BILIARY (CHOLANGIOLITIC CIRRHOSIS, HANOT HYPERTROPHIC CIRRHOSIS, CHRONIC NONSUPPURATIVE DESTRUCTIVE CHOLANGITIS, ETC.)
Other books
Semper Fidelis by S.A. McAuley, T.A. Chase, Devon Rhodes, LE Franks, Sara York, Kendall McKenna, Morticia Knight
CROSSFIRE by Jenna Mills
Ms. Hannah Is Bananas! by Dan Gutman
The Brenda Diaries by Margo Candela
A Splash of Red by Antonia Fraser
París era una fiesta by Ernest Hemingway
Keep You From Harm by Debra Doxer
Runt of the Litter (Halfbreed Chronicles Book 1) by Hemlock, Isabelle
The Great Quarterback Switch by Matt Christopher
Any Place I Hang My Hat by Susan Isaacs