Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (236 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
5.34Mb size Format: txt, pdf, ePub
Cystine stones are rare, occurring in patients with homozygous congenital familial cystinuria, and characterized by bilateral obstructive staghorn calculi with associated renal failure.
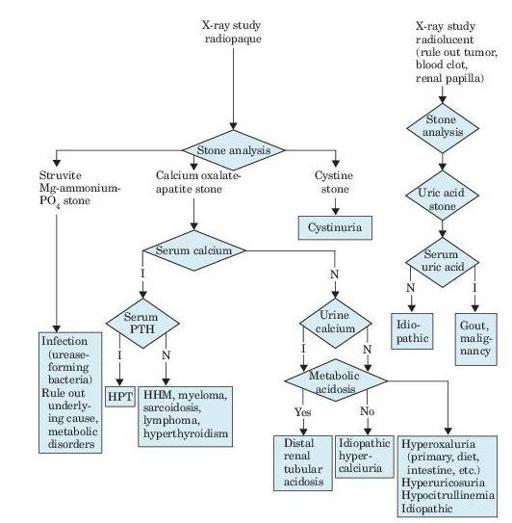
Figure 7–1
Algorithm for diagnosis of renal calculi, as revealed by flank pain, renal colic, hematuria, fever, and urinalysis findings. I, increased; N, normal; PTH, parathyroid hormone; HPT, hyperparathyroidism; HHM, humeral hypercalcemia of malignancy.
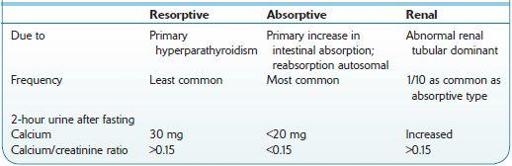
Table 7-1 Comparison of Types of Idiopathic Hypercalciuria
Who Should Be Suspected?
The waves or paroxysms of pain usually last 20–60 minutes and is related to the passage of the stone down the ureter and the associated ureteral spasm.
Other books
Slow Apocalypse by Varley, John
The Mile Long Spaceship by Kate Wilhelm
The Plantagenet Vendetta by Davis, John Paul
Kill Your Darlings by Max Allan Collins
Shadow Silence by Yasmine Galenorn
The Veritas Conflict by Shaunti Feldhahn
Absolute Power (Book 1): Origins by Queen, Grayson
Riding Hot by Kay Perry
Eastward Dragons by Andrew Linke
Julia London - [Scandalous 02] by Highland Scandal