Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (412 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
9.01Mb size Format: txt, pdf, ePub
THROMBOTIC THROMBOCYTOPENIC PURPURA/HEMOLYTIC UREMIC SYNDROME (TTP/HUS)
Definition
TTP and HUS are severe thrombotic microangiopathies characterized by systemic platelet aggregates causing ischemia in multiple organ systems, thrombocytopenia, and fragmentation of red cells. These conditions are expressed by microangiopathic hemolytic anemia, thrombocytopenia, and occasionally neurologic, and renal involvement. TTP and HUS are disorders with many similarities. There are, however, sufficient differences between these conditions to be considered separately.
TTP
Classically, patients with TTP were described as presenting with the following pentad: fever, microangiopathic hemolytic anemia, thrombocytopenia, and impaired renal and neurologic function. In reality, most patients have some, but not all, of the components of the pentad, and the pentad criteria are no longer used.
9-4
). The hereditary form, much less common, is known as the Upshaw-Schulman syndrome; it is the result of homozygous or compound heterozygous ADAMTS13 gene mutation.
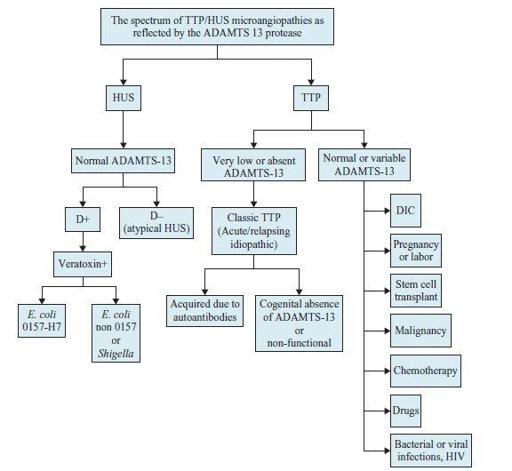
Figure 9–4
The spectrum of thrombotic thrombocytopenic purpura (TTP)/hemolytic uremic syndrome (HUS) microangiopathies as reflected by the ADAMTS 13 protease. E. coli, Escherichia coli.
HUS
E. coli
0157:H7 (most common cause in the United States) or
Shigella
(see Figure
9-4
). In different countries, other bacteria have been found to be the etiologic agent in HUS. HUS is a self-limited disease.
TTP
Other books
Captives (Nightmare Hall) by Diane Hoh
SexontheBeach by Amber Skyze
When Winter Bared Our Bones by Emily Asimov
Stolen Innocence by Erin Merryn
Death at Blenheim Palace by Robin Paige
The Secret Rooms: A True Gothic Mystery by Catherine Bailey
Assassins' Dawn by Stephen Leigh
Dead River by Cyn Balog
Hell Inc. by C. M. Stunich
Acid Lullaby by Ed O'Connor