Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (932 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
8.72Mb size Format: txt, pdf, ePub
A positive rapid fFN result may be observed for patients who have experienced cervical disruption caused by, but not limited to, events such as sexual intercourse, digital cervical examination, or vaginal probe ultrasound.
FIRST-TRIMESTER SCREENING
See Prenatal Screening.
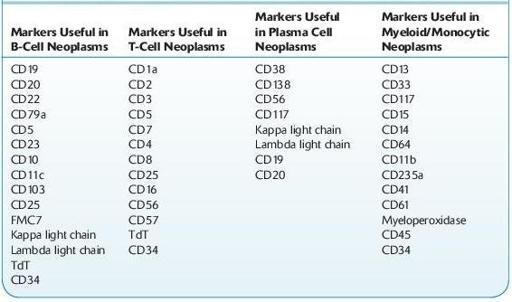
FLOW CYTOMETRY ANALYSIS IN THE CLINICAL EVALUATION OF HEMATOLOGIC DISEASES
*
Definition and use
Useful Flow Cytometric Immunologic Markers in Hematologic Neoplasms
Other books
The Daddy Decision by Donna Sterling
Christmas in Eternity Springs by Emily March
Nipped in the Bud by Susan Sleeman
Blessings of the Heart by Valerie Hansen
To Love a Way of Life by Natalie Hart
The Lake (The Lake Trilogy, Book 1) by Grant, AnnaLisa
Louisiana Laydown by Jon Sharpe
Supernova by Jessica Marting
Nowhere but Up by Pattie Mallette, with A. J. Gregory
Brothers Black: Wyatt the Heartbreaker by Blue Saffire