Breast Imaging: A Core Review (10 page)
Read Breast Imaging: A Core Review Online
Authors: Biren A. Shah,Sabala Mandava
Tags: #Medical, #Radiology; Radiotherapy & Nuclear Medicine, #Radiology & Nuclear Medicine

Answer choice A is incorrect because chemical shift artifact is an artifact that results from the different resonances of the hydrogen in fat and water. It is most commonly seen in non–fat-suppressed sequences (e.g., non–fat-suppressed T1-weighted) and results in signal void or bright signal at a fat–water interface. Answer choice C is incorrect because susceptibility artifact is usually due to metallic artifact(s) that appear(s) as signal voids on gradient echo sequences. On spin echo sequences, a signal flare component may be seen in addition to the signal void. Answer choice D is incorrect. There is no significant motion on this image. Motion artifact is one of the most commonly encountered artifacts affecting breast MRI. Motion can arise from patient motion or cardiac, respiratory, or great vessel motion. All motions propagate in the phase-encoding direction despite the direction of the motion. Phase-encoding direction should be left to right for axial sequences and superior to inferior for sagittal sequences to reduce the effect of cardiac and respiratory motion on the breasts.
53b
Answer A.
Increasing the number of sampling points in the phase-encoding direction or enlarging the FOV can correct phase wrap artifact.
Answer choice B is incorrect because reducing patient motion can prevent phase encoding or ghosting artifact. Answer choice C is incorrect because shimming the magnet (optimizing field homogeneity) of an MR imaging unit is performed to try to correct inhomogeneous fat saturation artifact. Answer choice D is incorrect because increasing bandwidth per pixel of the imaging sequence can reduce chemical shift artifact. Answer choice E is incorrect because checking the radiofrequency (RF) shield for a leak might be the cause for RF interference.
References: Harvey JA, Hendrick E, Coll JM, et al. Breast MR imaging artifacts: how to recognize and fix them.
Radiographics
2007;27:S131–S145.
Ojeda-Fournier H, Choe KA, Mahoney MC. Recognizing and interpreting artifacts and pitfalls in MR imaging of the breast.
Radiographics
2007;27:S147–S164.
54
Answer D.
The advantage of breast tomosynthesis is a reduction in overlapping tissue, which often obscures lesions on 2-D mammography, especially in patients with dense breast parenchyma. In digital breast tomosynthesis, images are acquired at different angles and are then reconstructed. This technique allows overlapping structures from different planes to be separated out. In digital breast tomosynthesis, compression is required to immobilize the breast. However, because digital breast tomosynthesis already reduces tissue overlap, the degree of compression potentially can be decreased; this is a topic of ongoing investigation.
References: Baker JA, Lo JY. Breast tomosynthesis: state-of-the-art and review of the literature.
Acad Radiol
2011;18(10):1298–1310.
Park JM, Franklin EA Jr, Garg M, et al. Breast tomosynthesis: present considerations and future applications.
Radiographics
2007;27:S231–S240.
55
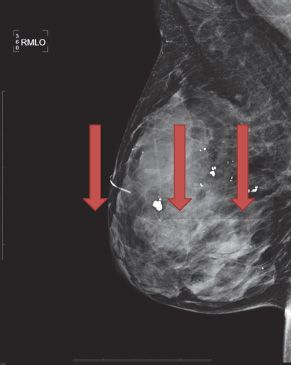
Answer A.
The mediolateral oblique view shows a detector interface line (see
red arrows
in image below) from a selenium-based detector. This artifact is due to a slight difference in calibration of two halves of the detector and relatively high exposure for imaging a very dense breast tissue.
Reference: Geiser WR, Haygood TM, Santiago L, et al. Challenges in mammography: part 1, artifacts in digital mammography.
AJR Am J Roentgenol
2011;197(6):W1023–W1030.
| 2 | Breast Cancer Screening |
QUESTIONS
1
Which is an American Cancer Society (ACS) recommendation, based on evidence from nonrandomized screening trials and observational studies, for performing a screening breast MRI as an adjunct to mammography?
A. Heterogeneously or extremely dense breast on mammography
B. Women with a personal history of breast cancer, including ductal carcinoma in situ (DCIS)
C. Lifetime risk 15% to 20%, as defined by BRCAPRO or other models that are largely dependent on family history
D. First-degree relative of
BRCA
carrier but untested
E. Lobular carcinoma in situ (LCIS) or atypical lobular hyperplasia (ALH)
2
Regarding the structure marked in the image below, which of the following statements is correct?
A. Described as cigar shaped
B. Present in males and females
C. Seen on the CC and true lateral projections only
D. Associated with tubular carcinoma
3a
A 61-year-old female presents for a screening mammogram. Patient’s most recent prior mammogram from 2 years ago was negative. What is the most appropriate BI-RADS classification based on this single right MLO view?

A. 0
B. 2
C. 3
D. 4
E. 5
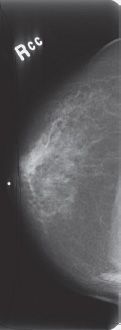
3b
Additional views were performed. What is the most appropriate description of these calcifications?
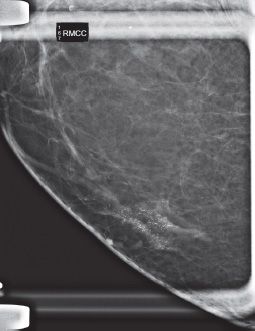
A. Fat necrosis (dystrophic, rim, and lucent centered)
B. Pleomorphic, fine linear branching
C. Skin calcifications
D. Coarse/popcorn-like
E. Rod-like/secretory
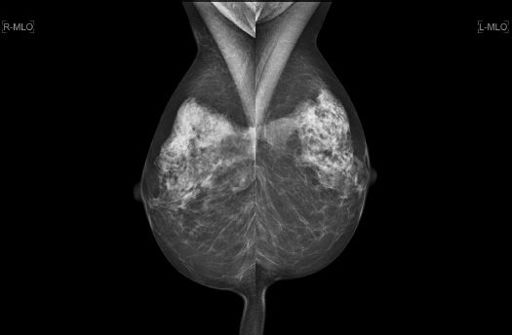
4
A 62-year-old female presents for her annual routine screening mammogram. The interval between the two studies is 13 months. The patient has no current complaints. Comparing the current study with the prior, what is the MOST likely cause of the change in her mammogram in the interval?


A. Hormone replacement therapy
B. Weight loss
C. Inflammatory breast cancer
D. Breast edema from congestive heart failure
5
A 57-year-old female presents for an annual routine screening mammogram. Which of the following statements is correct regarding this patient’s prior breast surgical history?
Other books
The House of the Scorpion by Nancy Farmer
A Brilliant Novel in the Works by Yuvi Zalkow
Soldier for the Empire by William C Dietz
Better Unwed Than Dead by Laura Rosemont
Travellers in Magic by Lisa Goldstein
Amaretto Flame by Sammie Spencer
Score! by Jilly Cooper
creepy hollow 05 - a faerie's revenge by morgan, rachel
Without Faith by Leslie J. Sherrod
The Wolf's Prey by Edugardo Gilbert X