Pediatric Primary Care (71 page)

Figure 24-7b
Stepwise approach for managing asthma in children 5–11 years of age.
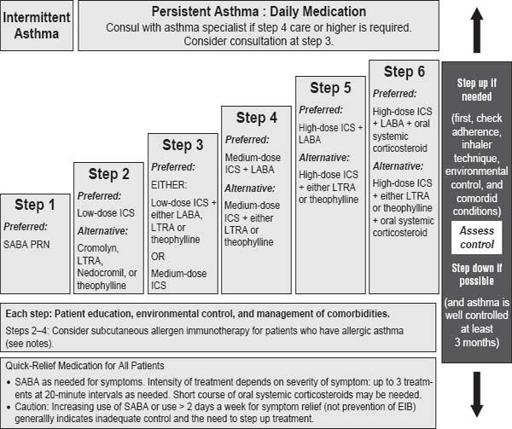
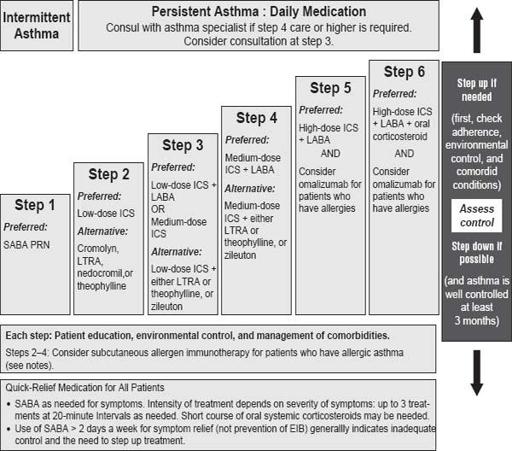
Figure 24-8
Stepwise approach for managing asthma in youths ≥ 12 years of age and adults.
BIBLIOGRAPHY
Behrman R, Kliegman R, Jenson H.
Nelson textbook of pediatrics.
17th ed. Philadelphia, PA: W.B. Saunders; 2004.
CDC fact sheet: influenza technical information.
Atlanta, GA: Centers for Disease Control and Prevention; 2003.
CDC fact sheet: pertussis technical information.
Atlanta, GA: Centers for Disease Control and Prevention; 2003.
Klassen T, et al. Nebulized budesonide and oral dexamethasone for treatment of croup: a randomized controlled trial.
J Am Med Assoc.
1998;279(20):1635.
Long S, Pickering L, Prober C.
Principles and practice of pediatric infectious diseases.
2nd ed. Philadelphia, PA: Churchill Livingstone; 2003.
Michael M. Scope and impact of pediatric asthma.
NursePract.
2002;27(S):7.
National Heart, Lung, and Blood Institute, Global Initiative for Asthma.
Global burden of asthma
(NIH Publication No 02-3659:3) Bethesda, MD: National Institutes of Health; 2003.
National Heart, Lung, and Blood Institute, National Asthma Education and Prevention Program.
NAEPP expert panel report guidelines for the diagnosis and management of asthma, update on selected topics 2002
(NIH Publication No 02-5075). Bethesda, MD: National Institutes of Health; 2002.
National Heart, Lung, and Blood Institute, National Asthma Education and Prevention Program.
Practical guide for the diagnosis and management of asthma
(NIH Publication No 97-4053). Bethesda, MD: National Institutes of Health; 1997.
Pickering L. Influenza diagnosis and treatment in children: a review of studies on clinically useful test and antiviral treatment for influenza.
Pediatr Infect Dis J.
2003;22(2):170.
Pickering L.
Red book.
26th ed. Elk Grove Village, IL: American Academy of Pediatrics; 2003; p. 383.
Storch G. Rapid diagnostic tests for influenza.
Curr Opin Pediatr.
2003;15:79.
Taussig M, Landau L.
Pediatric respiratory medicine.
St. Louis: Mosby; 1999; p. 565.
CHAPTER 25
Cardiovascular Disorders
Karen M. Corlett
I. CHEST PAIN
| Asthma, 493.81 | Musculoskeletal, 786.59 |
| Asthma, exercise-induced, 493.9 | Myocarditis, 429 |
| Cardiac murmur, 782.2 | Obesity, 278 |
| Cardiomegaly, 429.3 | Palpitations, 785.1 |
| Cardiomyopathy, 425.4 | Pericarditis, 423.9 |
| Chest pain, 786.5 | Pneumonia, 486 |
| Chest pain, noncardiac, 786.59 | Pneumothorax, 512.8 |
| Congenital heart disease, 746.9 | Presyncope, 780.2 |
| Congestive heart failure, 428 | Pulmonary, 786.52 |
| Coronary artery anomalies, 746.9 | Pulmonary embolus, 415.19 |
| Coronary artery disease, 414.9 | Rheumatic fever, 391.9 |
| Dizziness, 780.4 | Supraventricular tachycardia, 427.89 |
| Dysrhythmias, 427.9 | Syncope, 780.2 |
| Enlarged liver, 789.1 | Tachycardia, 785 |
| Gastroesophageal refl ux, 530.81 | Tachypnea, 786.06 |
| Heart disease, acquired, 429.9 | Turner syndrome, 758.6 |
| Heart murmur, 785.2 | Valvular defects, 424 |
| Kawasaki disease, 446.1 | Ventricular tachycardias, 427.1 |
| Marfan syndrome, 759.82 | Weak peripheral pulses, 785.9 |
A. Etiology.
1. Classes of chest pain.
a. Severe, acute, unremitting chest pain: Refer immediately to pediatrician or urgent/emergent care facility. Rare and most often due to cardiac, pulmonary, or gastrointestinal causes.
b. Chronic or recurrent chest pain: more likely.
• Typically patient has had several episodes of chest pain before medical attention is sought.
• Many times, physical exam may be normal.
• Patient history is crucial in elucidating etiology of chest pain although large percentage of chest pain in children will never have etiology determined.
• Chest pain is distressing to patients, families: chest pain in adult friends, relatives typically signifies cardiac event, most chest pain in childhood is noncardiac in origin.
• Thorough history and physical can rule out serious causes for chest pain.
2. Chest pain, cardiac in origin.
a. Coronary artery disease.
b. Congenital heart disease.
c. Typically have murmur.
d. Acquired heart disease.
e. Infectious etiologies.
f. Cardiomyopathy, pericarditis, Kawasaki disease, rheumatic fever.
g. Myocardial issues, myocarditis.
h. Cardiomyopathies.
i. Dysrhythmias.
j. Supraventricular or ventricular tachycardias.
3. Chest pain, noncardiac in origin: most common.
a. Musculoskeletal.
b. Pulmonary.
c. Gastrointestinal.
d. Psychogenic.
B. Occurrence.
1. Few studies of overall incidence of chest pain in pediatric population due to wide range of specialists to whom these patients are referred.
2. Incidence, particularly in adolescents, is significant.
C. Clinical manifestations.
1. Chronic or recurrent intermittent chest pain.
a. Most often occurs in adolescent population.
b. May or may not limit activities.
c. Usually chest pain has been long standing before treatment is sought.
d. Important to elucidate inciting factors and relieving factors.
• Relationship of pain to activity varies.
e. Associated symptoms.
• Syncope, presyncope, dizziness, palpitations.
Other books
The Interior Castle by Ann Hulbert
State of Pursuit by Summer Lane
Stand (Black Addiction Book 3) by T Gephart
Hadley (The Club Girl Diaries Book 3) by Addison Jane
'Tis the Season to Get Lucky (Entangled Indulgence) by Rice, Heidi
The Captives of Kaag by Joe Dever
All the Truth That's in Me by Julie Berry
The Art of Forgiving - A Uni File Short (The Uni Files) by Bloom, Anna
Paradise Park by Iris Gower
The Duchess Who Wouldn't Sit Down by Jesse Browner