Resident Readiness General Surgery (35 page)
Read Resident Readiness General Surgery Online
Authors: Debra Klamen,Brian George,Alden Harken,Debra Darosa
Tags: #Medical, #Surgery, #General, #Test Preparation & Review

3.
ICU patients are almost always imaged supine and are not able to take deep inspirations. Low lung volumes and portable technique significantly impair the ability to evaluate the lung parenchyma. Therefore, the most important function of the ICU chest x-ray is to identify tubes, lines, and drains and assure that they are in the proper positions. Three of the most important items you will use a CXR to assess include endotracheal tubes, esophagogastric tubes (including orogastric and nasogastric tubes), and central venous catheters (see
Figure 25-2
).
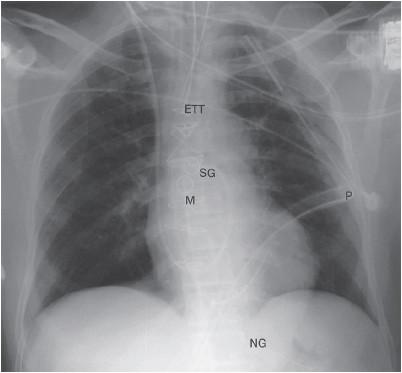
Figure 25-2.
Frontal radiograph immediately after coronary artery bypass surgery shows typical lines and tubes encountered in the ICU. Endotracheal tube (ETT), nasogastric tube (NG), Swan-Ganz catheter (SG), mediastinal drain (M), and left pleural drain (P) are present.
Endotracheal tubes: The ideal position for an endotracheal tube is in the midtrachea, 3 to 5 cm from the carina when the head is neither flexed nor extended. The carina is the upside down V where the trachea splits into the left and right mainstem (see
Figure 25-1
). The minimum safe distance from the carina is 2 cm.
Esophagogastric tubes: Make sure the tube tracks down the esophagus and goes below the diaphragm into the stomach. A tube that does not make it all the way to the stomach should be advanced and the CXR retaken. A tube that makes a turn and stays above the diaphragm could be placed into the lung—you must replace the tube. Also check that the side hole is below the diaphragm. If it isn’t, giving tube feeds can cause aspiration pneumonia as fluid may reflux back up the esophagus. In patients who are very tall it is often difficult to see the tip of the tube and a KUB may be necessary (see
Figure 25-2
).
Central venous catheter (CVC): Central venous catheters include those that terminate in the SVC or IVC. They may be placed through the neck/chest (internal jugular/subclavian veins), arm (PICC lines), or even lower extremities. They can be used to monitor central venous pressure, infuse large volumes of fluid, and infuse caustic medications that cannot be given through a peripheral vein. The optimal position for a CVC is for the tip to be right at the cavoatrial junction. As the right superior heart border is not a reliable determinant of right atrial position, the best way to confirm correct placement is to look for the tip to be at the junction of the right heart border with the right mainstem bronchus. Catheters should always go toward the heart: catheters inserted from the left should cross midline and end up on the right side near the right atrium. When right-sided catheters cross midline, intra-arterial rather than intravenous placement should be suspected (see
Figure 25-3
).
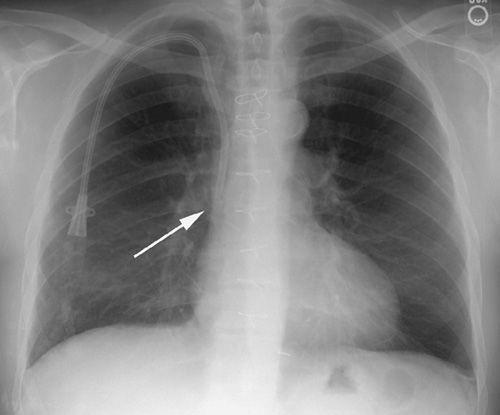
Figure 25-3.
PA view of a patient whose tunneled central venous catheter placement is normal with its tip in the superior vena cava above the right atrium (arrow).
TIPS TO REMEMBER
The best system for reading a chest x-ray is the one that you can remember easily and that helps you to remember to look for all important features.
COMPREHENSION QUESTIONS
1.
What is the most important system to read a CXR?
A. The one that works best for you
B. The one in this book
C. The one you were taught in medical school
D. The one the Chief of Radiology uses
2.
Where should the tip of the endotracheal tube lie?
A. Below the diaphragm
B. Above the clavicles
C. 3 to 5 cm above the carina
D. Anywhere as long as the oxygen saturation is 100%
3.
Which of the following does
not
represent a problem with central venous catheter placement?
A. A right-sided pneumothorax after a right subclavian line placement
B. A left subclavian line with the tip in the jugular vein
C. A right-sided catheter that crosses midline
D. A left-sided catheter that crosses midline
Answers
1.
A
. It is imperative that you develop your own system to consistently and accurately read chest x-rays.
2.
C
. The tip of the endotracheal tube should be positioned 3 to 5 cm above the carina. Any further and you risk the tube sliding into a mainstem bronchus with neck extension.
3.
D
. A left-sided catheter should cross the midline. The other choices represent serious problems with placement.
 A 65-year-old Woman in Respiratory Distress
A 65-year-old Woman in Respiratory Distress
Alden H. Harken, MD and Brian C. George, MD
Ms. O’Sullivan is a 65-year-old woman who arrived in the PACU 30 minutes ago following a right colectomy. She was extubated in the operating room. Her vitals are: BP 140/90, pulse 120 (regular), respiratory rate 30, temperature 37.5°C, and finger oximetry 80%. She is anxious and agitated and says that she wants to “leave right now and go home.”
1.
Until proven otherwise, what is the cause of agitation and/or disorientation in the postoperative recovery unit?
2.
Explain several causes of postoperative hypoxemia.
3.
What are the indications to intubate a patient?
RESPIRATORY DISTRESS
If you are sitting comfortably reading this chapter, you are using about 3% of your energy in the work of breathing. Interestingly, the “driver” of this lung work is blood acidosis (actually CSF hydrogen ion concentration)—not oxygen. You are exquisitely sensitive to P
CO
2
/pH. If you hold your breath for a minute, at the end of that minute your only wish is for another breath—breathing is high on everyone’s list of fun things to do. However, at the end of a minute of apnea, your P
CO
2
has risen from 40 mm Hg to only about 48 mm Hg. Therefore, a relatively tiny decrease in arterial pH (or increase in P
CO
2
) translates into a profound stimulus to breathe.
Case Analysis
Mrs. O’Sullivan’s respiratory rate has increased to 30. We could attribute this to her “agitation,” but were we to check her arterial blood gas at this time, we would find:
P
O
2
: 55 mm Hg
P
CO
2
: 30 mm Hg
pH: 7.48
O
2
sat: 80%
She has a respiratory alkalosis and is actually “overbreathing.” Her only abnormality is the drop in her hemoglobin saturation (O
2
sat) that confers a 20% (100% minus 80%) decrease in arterial oxygen content, which can be completely
compensated by a 20% increase in her cardiac output, resulting in a rock stable systemic oxygen delivery. The patient’s agitation has unquestionably pumped up her cardiac output at least the necessary 20%—so, what’s the problem? You decide that “everything is fine,” so you reassure the patient and the nurses and leave to check on another patient.
Answers
1.
Fifteen minutes later you get a call that Mrs. O’Sullivan is climbing out of bed, making a lot of noise, and bothering the other patients (and the nurses)—so, “Can we sedate her?”
Warning: if you depress this patient’s respiratory drive with a sedative now, you will receive a follow-up call in 30 minutes that she just suffered a cardiac arrest.
Agitation/irritability/confusion in the PACU/ICU is hypoxemia until proven otherwise, and should be cause for alarm!
In most of us, the symptoms of hypoxemia are not an alteration in breathing volume/rate/pattern. Acute hypoxemia just makes a patient feel anxious and restless. Hypoxemia makes a patient want to get up, go out, and travel to someplace safer—and hypoxemic patients are very likely to announce this desire to everyone.
2.
There are lots of reasons for hypoxemia in the early postoperative period. Atelectasis, aspiration, a touch of pneumonia, and even a pulmonary embolus are the most obvious reasons that ventilation doesn’t match up with perfusion. More fundamental is that most inhalational anesthetics block hypoxic pulmonary vasoconstriction. Remember, this is the unique capability of the pulmonary arterioles to divert perfusion away from hypoventilated alveoli. When poorly ventilated lung is perfused, a shunt occurs that results in hypoxemia.