Resident Readiness General Surgery (60 page)
Read Resident Readiness General Surgery Online
Authors: Debra Klamen,Brian George,Alden Harken,Debra Darosa
Tags: #Medical, #Surgery, #General, #Test Preparation & Review

Imaging studies may be useful but only in those instances where the patient is not decompensating and the diagnosis remains equivocal. Plain radiographs may show gas within soft tissues, although this is only present in one third of patients and a negative study cannot rule out NSTI. There are some data that suggest CT scans, with or without contrast, may be helpful in identifying characteristic features of NSTIs such as soft tissue gas and inflammatory changes. Although CT scans may have a role in diagnosing NSTIs, this has not yet been adequately studied. MRI has been shown to have a sensitivity of 90% to 100% in diagnosing NSTIs, but a specificity of only 50% to 80%. Because MRIs take such a considerable amount of time to obtain, the risks associated with delaying treatment drastically limit the utility of MRI in the evaluation of NSTIs. For examples of imaging studies that demonstrate NSTIs, see
Figure 45-2
.
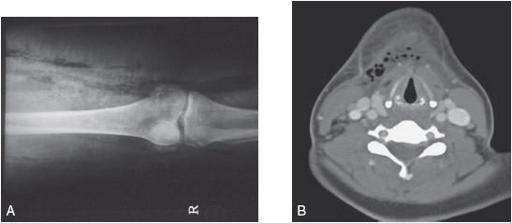
Figure 45-2.
Radiographic evidence of necrotizing soft tissue infections. (
A
) Plain radiograph that demonstrates gas in the soft tissue of the right lower extremity. (Courtesy of Susan Dufel, MD.) (
B
) CT scan demonstrating gas within the soft tissue of the neck as well as fat stranding that crosses fascial planes. (Reproduced, with permission, from Tintinalli JE, Stapczynski JS, Ma OJ, et al.
Tintinalli’s Emergency Medicine
. 7th ed. New York: McGraw-Hill; 2011. Figure 241-5.)
The gold standard in the diagnosis of NSTI is operative exploration. Operative findings consistent with necrotizing infection include tissue necrosis, lack of bleeding, foul-smelling discharge, and loss of normal fascial resistance to finger dissection. When there is any level of concern for NSTI and especially if a patient is showing signs of rapid clinical deterioration, the patient should be emergently taken to the operating room for exploration. The consequences of not doing so are far more severe than those associated with a negative exploration.
Treatment
The treatment of NSTIs is based on four key principles: (1) immediate surgical debridement; (2) fluid resuscitation and correction of electrolyte and acid–base abnormalities; (3) antimicrobial therapy; and (4) support of failing organ systems.
Early surgical debridement, as previously discussed, is the mainstay of treatment and has been shown to increase survival. Fluid resuscitation with crystalloids is necessary, as nearly all patients with NSTIs have intravascular volume depletion. Lactated Ringer’s solution is the crystalloid of choice since it is common for these patients to be acidotic. Electrolyte abnormalities should be corrected in the usual fashion. Antimicrobial therapy should be started immediately in cases of NSTI. Although they do not penetrate necrotic tissue and thus are not curative, they do decrease the systemic symptoms of infection and are an important adjuvant therapy. Given the rapid progression and extremely high morbidity and mortality associated with NSTIs, initial antibiotic coverage should be broad until culture results are available. Clindamycin should also be included in the initial antibiotic regimen, as it decreases the toxin production by
Staphylococcus aureus
, hemolytic
Streptococcus
, and
Clostridium
infections. Lastly, providing support for failing organ systems is essential in the ICU setting.
In summary, if you have any suspicion that a wound infection might be an NSTI, you should examine the wound closely, removing the original operative dressing if necessary. If you remain concerned about an NSTI, you must immediately notify your senior resident or attending in order to expedite the diagnostic workup and/or the possible emergency operation. While you wait for the resident or attending to call you back, you should start IV fluids and a broad-spectrum empiric antibiotic regimen that includes clindamycin.
TIPS TO REMEMBER
NSTIs can widely vary in presentation. Concerning findings include pain out of proportion to the exam, diaphoresis, woody edema, crepitus, bronzing of skin, dishwater discharge, skin necrosis, bullae formation, unexplained fever, and hypotension.
3
or a sodium level <135 mmol/L on admission to the hospital has an 80% positive predictive value and, if not present, an 80% negative predictive value in individuals with NSTI.
COMPREHENSION QUESTIONS
1.
You are performing a postoperative check on a trauma patient who just underwent an exploratory laparotomy after a motorcycle crash. He tells you that he is having severe pain in his right leg, where there was a “road rash” that was previously cleaned and dressed. You remove the bandage on his thigh and discover that
the previously minor wound now has 2 to 3 cm of surrounding erythema. On palpation, you notice he has extreme tenderness beyond the margins of the erythema and you notice some crepitus. You suspect NSTI. What should be your next step?
A. Send a BMP to check his serum sodium level.
B. Wake up your senior resident and inform her of your findings.
C. Come back and reevaluate the wound in 2 to 3 hours.
D. Culture the wound.
E. Order a stat MRI of the right lower extremity.
2.
Which of the following are key principles in the management of NSTIs?
A. Immediate surgical debridement
B. Supporting failing organ systems
C. Fluid resuscitation
D. Correction of electrolyte and acid–base abnormalities
E. Antimicrobial therapy
F. A, C, E
G. All of the above
Answers
1.
B
. Any time that an NSTI is suspected, it is essential to notify senior members of the surgical team immediately. NSTIs are surgical emergencies and should be approached with the same level of urgency as a trauma or an acute abdomen. Cultures would not be immediately useful in this case, as NSTI is a clinical diagnosis that must be debrided before cultures would have time to come back. Although MRI can aid in the diagnosis of NSTIs, it is time consuming and is not justified—a negative operative exploration is perfectly acceptable in this case.
2.
G
. All of these options are key principles in managing NSTIs.
 A 35-year-old Man With Crohn Disease Who Needs Postoperative Orders
A 35-year-old Man With Crohn Disease Who Needs Postoperative Orders
Roy Phitayakorn, MD, MHPE (MEd)
You are taking care of a 35-year-old man with Crohn’s disease. His symptoms were somewhat controlled with 30 mg of oral prednisone daily, but he developed a chronic, long-segment ileal stricture that required an open ileocolectomy with primary anastomosis. You are writing his postoperative orders.
1.
What is the mechanism of acute adrenal insufficiency?
2.
Should you have given him a “stress” dosage of steroids at the start of the case? Why or why not?
3.
How do you determine how much steroids to give for stress dosages?
4.
How much steroid should he have postoperatively and how fast can you taper this stress dose?