Resident Readiness General Surgery (56 page)
Read Resident Readiness General Surgery Online
Authors: Debra Klamen,Brian George,Alden Harken,Debra Darosa
Tags: #Medical, #Surgery, #General, #Test Preparation & Review

COMPREHENSION QUESTIONS
1.
Which acid–base disturbance can occur with large-volume infusions of NS?
A. Anion gap metabolic acidosis
B. Metabolic alkalosis
C. Respiratory acidosis
D. Non-anion gap metabolic acidosis
2.
What is the appropriate solution to use for large intestine (diarrheal) losses?
A. LR with potassium
B. LR with bicarbonate
C. NS with chloride
D. NS with bicarbonate
3.
To obtain the same theoretical increase in plasma volume, what ratio of crystalloid to colloid solution is needed for 0.45 (ie, 0.5) NS compared with albumin?
A. 1:1
B. 3:1
C. 6:1
D. 10:1
Answers
1.
D
. Non-anion gap metabolic acidosis results from the large infusion of chloride ions.
2.
A
. The large intestine has a high potassium concentration and so this is the electrolyte that needs to be replaced with diarrheal losses. LR contains potassium, but NS with added potassium can also be used.
3.
C
. 0.45% NS is also known as 0.5 NS. Since it is half the tonicity of 0.9% NS, you must double the 3:1 ratio described above.
 A 68-year-old Woman With Electrolyte Abnormalities
A 68-year-old Woman With Electrolyte Abnormalities
Molly A. Wasserman, MD and Mamta Swaroop, MD, FACS
Ms. Jones is a 68-year-old female with a past medical history significant for hypertension and hyperlipidemia, now 2 years status post open sigmoidectomy for recurrent diverticulitis. She presents with a 3-day history of crampy abdominal pain, nausea, and 5 episodes of nonbloody, nonbilious emesis. She also reports a gradual onset of abdominal distension with obstipation. Her last bowel movement was 4 days ago and was normal. She has had associated anorexia and subjective fevers. Her medications include furosemide and atorvastatin.
On physical exam, her vitals are as follows—T: 101.5; HR: 120; BP: 140/90; RR: 16; O
2
: 99% on RA; and weight: 70 kg. Abdominal exam reveals absent bowel sounds, abdominal distension with diffuse tympany, and tenderness in the left upper and lower quadrants with no rebound or guarding. The remainder of the exam is normal. Labs are notable for a sodium level of 130, potassium of 2.8, and magnesium of 1.5.
1.
Why are Mrs. Jones’ electrolytes abnormal?
2.
What are the risks associated with leaving her sodium and potassium uncorrected?
3.
What orders would you write to replete her potassium?
ELECTROLYTE ABNORMALITIES
The ability to anticipate electrolyte abnormalities is of paramount importance in the treatment and management of the surgical patient. It will also be one of your primary responsibilities as a surgical intern. You will be expected to take care of all but the most severe abnormalities. It is important to know when and how to replace electrolytes, and when to alert the senior on service in the case of a severe and potentially life-threatening abnormality.
Answers
1.
Fluids and electrolytes can be lost most commonly from the gastrointestinal tract (emesis, diarrhea, nasogastric tubes, enterocutaneous fistulas), from the genitourinary system (renal disease), from the skin (sweat, burns, fever), and from fluid shifts (third spacing, postoperative open abdomens, vacuum-assisted wound closure devices, hemorrhage). Electrolyte abnormalities may be worsened by a patient’s NPO status and the administration of intravenous fluids that
are insufficient to meet the patient’s metabolic demands. Predicting losses and repleting the patient early is the best way to thwart electrolyte abnormalities. In the case above, this patient has had both diarrhea and emesis, most likely has not been able to replete her losses secondary to anorexia, and will be made NPO and receive a nasogastric tube as part of her initial treatment. All of these factors compound each other to cause this patient to be at high risk of having severe electrolyte abnormalities. Additional consideration must be given to the patient’s medications. As an example, loop diuretics (eg, furosemide) put the patient at risk of hypokalemia.
2.
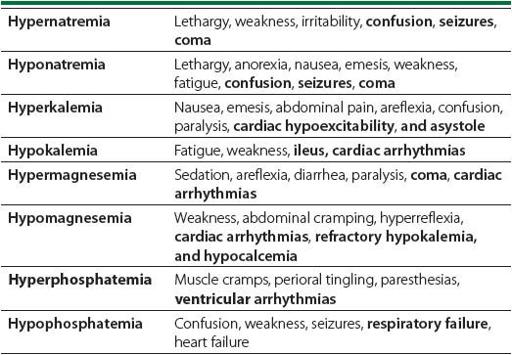
Table 43-1
depicts the common symptoms and signs of electrolyte abnormalities. As shown below, electrolyte disorders have a wide range of symptoms. Common among these are a delayed return of bowel function, muscle weakness and fatigue, cardiac dysfunction and dysrhythmias, seizures, and failure to wean from a ventilator.
Table 43-1.
Symptoms and Signs of Electrolyte Abnormalities
3.
It is important to memorize how to treat each of the most common electrolyte abnormalities.
Hyponatremia
: Hyponatremia is defined as a serum sodium concentration <135 mEq/L. There are a variety of causes of hyponatremia in the surgical patient. ADH is elevated as a part of the normal stress response, and activation of inflammatory and stress cytokines (IL-1, IL-6, TNF-α) further increases ADH release. Fluid overload, high-output enterocutaneous fistulas, and aggressive diuresis may also result in hyponatremia. Initial treatment of hyponatremia involves determination of the sodium deficit and overall volume status:

where TBW = 0.6 × (weight in kg) for male and TBW = 0.55 × (weight in kg) for female.
In treating hyponatremia, it is important to determine the overall fluid status of the patient. Hypovolemic, hyponatremic patients can often be treated by rehydration with normal saline or Lactated Ringer’s solution. Conversely, euvolemic or hypervolemic patients who are asymptomatic are best initially treated with free water restriction. Symptomatic patients require administration of hypertonic saline. Overly aggressive treatment of hyponatremia will result in central pontine myelinolysis and possible permanent spastic quadriparesis and pseudobulbar palsy. As such, serum sodium should be repleted at a rate of <8 mEq/kg/day or 0.25 mEq/L/h.
Hypernatremia
: Hypernatremia is defined as a serum sodium concentration of >145 mEq/L. It is less common in the surgical patient but may be seen in patients with increased insensible water losses (burns, tracheostomies), major GI losses (NG tube suction, diarrhea, emesis), administration of sodium (TPN, sodium bicarbonate infusion), and when hypotonic losses are replaced with isotonic solutions (eg, post resuscitation). As with hyponatremia, the initial step in the treatment of hypernatremia is determining the free water deficit:

Patients with severe (Na >160 mEq/L) or symptomatic hypernatremia should be treated with D5W or D5 0.45 NS to correct at a rate of less than 0.5 mEq/L/h. Once the free water deficit is calculated, the first half of the total deficit should be administered over the first 24 hours, and the second half over the subsequent 24 hours. Overly rapid correction may result in cerebral edema and brainstem herniation.
Hypokalemia
: Potassium is the dominant intracellular cation, and only 2% of total body potassium resides in the serum. Potassium balance is controlled by the renin–angiotensin–aldosterone axis. Hypokalemia is defined as a serum potassium concentration <3.5 mEq/L. Total body potassium levels may be depleted by decreased potassium intake, increased loss from the GI tract (NG tube, emesis, diarrhea), renal disease, catecholamine stimulation, and certain medications (insulin, diuretics). Signs and symptoms of hypokalemia include gastrointestinal ileus, generalized fatigue and weakness, cardiac arrhythmias, and renal insufficiency. ECG abnormalities include flattened T waves, depression of ST segments, prominent U waves, and prolongation of the QT interval (
Figure 43-1
).
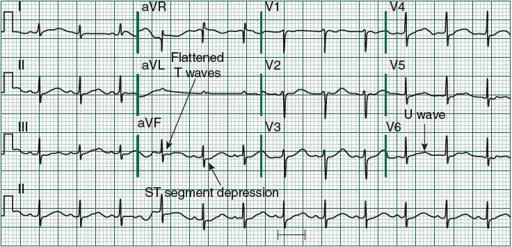
Figure 43-1.
ECG abnormalities seen in hypokalemia. (Modified, with permission, from Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J.
Harrison’s Principles of Internal Medicine
. 18th ed. New York: McGraw-Hill; 2012. Figure e28-24. <
www.accessmedicine.com
>. Copyright © The McGraw-Hill Companies, Inc. All right reserved.)