Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (1347 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
6.89Mb size Format: txt, pdf, ePub

Epstein-Barr nuclear antigen:
Last antibodies to appear and are rare in acute phase; develops 4–6 weeks after onset of clinical illness and rises during convalescence (3–12 months) and persists for many years after illness. Absence when IgM-VCA and anti-D are present implies recent infection. Appearance early in illness excludes primary EBV infection. Appearance after previous negative test evidences recent EBV infection.
Use
Diagnosing IM. In patients with suspected IM and a negative heterophile test.
Table
17-1
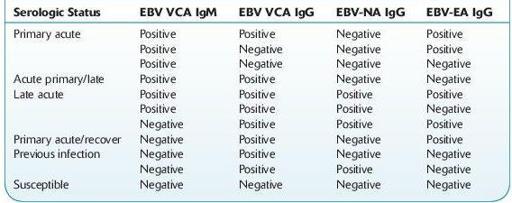
TABLE 17–1. Interpretation of Epstein-Barr Virus (EBV) Serologic Status
ESCHERICHIA COLI
(ENTEROHEMORRHAGIC, SHIGA TOXIN– PRODUCING
E
.
COLI
, STEC,
E
.
COLI
O157:H7) CULTURE (RULE OUT)
Other books
Deadeye Dick by Kurt Vonnegut
The Gift of Asher Lev by Chaim Potok
On Deadly Ground (Dan & Chloe Book 2) by Flamank, Nathan L.
Crossing Boundaries (Cape Falls) by Crescent, Sam
Family Drama 4 E-Book Bundle by Pam Weaver
The Bat by Jo Nesbo
The Soldier by Grace Burrowes
Betrayal by Lady Grace Cavendish
Unclean by Byers, Richard Lee