Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (157 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
4.83Mb size Format: txt, pdf, ePub
The patient may present with stigmata of chronic blood loss (
iron deficiency
anemia and related symptoms) or acute blood loss (weakness or syncope).
Screening
: Currently, screening for asymptomatic ulcerated lesions of the GI tract is generally recommended, especially for carcinoma of the colon and large adenomas.
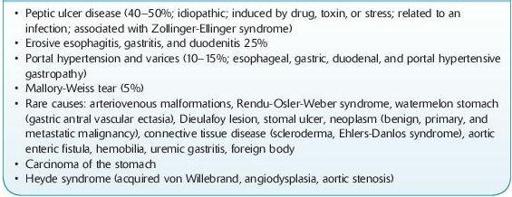
Differential Diagnosis of Upper Gastrointestinal Bleeding (Table
5-3
)
PUD (see discussion of acute abdomen under Abdominal Pain) (40–50% of patients) is associated with risk factors including
H. pylori
infection, use of NSAIDs, stress, and increase of gastric acid. It accounts for gastritis in 10% of patients, esophagitis 6% associated with gastric reflux (GERD). Risk factors for stress-related bleeding include respiratory failure and coagulopathy. Portal hypertension and varices (18% of patients) indicate the severity of a patient’s underlying cirrhosis. These patients have an associated mortality of 50% even after control of the hemorrhage.
TABLE 5–3. Differential Diagnosis of Upper Gastrointestinal Bleeding
Other books
Billionaire Badboy by Kenzie, Sophia
Questions About Angels by Billy Collins
The Rancher's First Love by Brenda Minton
Murder Most Unladylike: A Wells and Wong Mystery by Robin Stevens
Emaús by Alessandro Baricco
Red Madrassa: Algardis #1 by Edun, Terah
The Vast Fields of Ordinary by Nick Burd
Prey by cassanna dwight
Bilgewater by Jane Gardam
Tangling with the Tiger: Lone Pine Pride, Book 5 by Vivi Andrews