Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (229 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

The main goal of hypercalcemia workup is to differentiate PTH-mediated hypercalcemia from non–PTH-mediated hypercalcemia.
Interpretation of serum calcium. Approximately 40–50% protein bound (predominantly to albumin), but only the ionized or free of the circulating calcium concentration is physiologically important. Hypercalcemia is caused by an elevation in the ionized or free calcium concentration. In patients with hypo- or hyperalbuminemia, the measured calcium concentration should be corrected for abnormality in albumin. Pseudohypercalcemia should be excluded; it is related to increased protein binding due to either severe dehydration and hyperalbuminemia or production of calciumbinding paraprotein in patients with multiple myeloma. On the contrary, in patients with hypoalbuminemia due to chronic illness or malnutrition, total serum calcium concentration may be normal when serum ionized calcium is elevated.
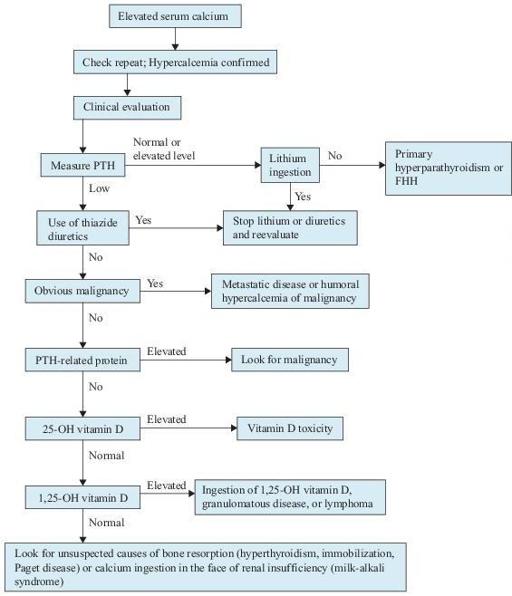
Figure 6–14
Algorithm for the workup of hypercalcemia. FHH, familial hypocalciuric hypercalcemia; PTH, parathyroid hormone.
TABLE 6–8. Laboratory Results in Common Causes of Hypercalcemia
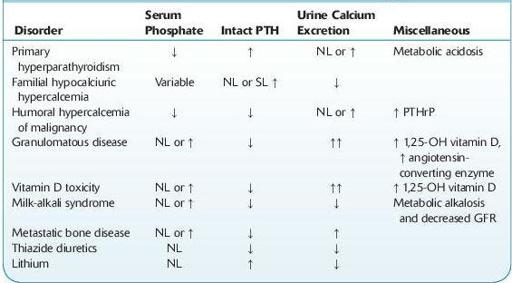
NL, normal level; PTHrP, parathyroid hormone–related protein; SL, slightly.
Normal values: urine calcium: 100–250 mg/24 h (females) and 100–300 mg/24 h (males); serum phosphate: 2.5–4.5 mg/dL; PTH (intact): 12–72 pg/mL; 1,25-OH Vitamin D: 14–78 pg/mL; angiotensin-converting enzyme: 17–70 units; PTHrP: <2.8 pmol/L.
Suggested Readings
Agus ZS. Clinical manifestations of hypercalcemia. In: Rose B, (ed).
UpToDate
, Waltham, MA: UpToDate, Inc.; 2009.
Agus ZS. Diagnostic approach to hypercalcemia. In: Rose B, (ed).
UpToDate
, Waltham, MA: UpToDate, Inc.; 2009.
Agus ZS. Etiology of hypercalcemia. In: Rose B, (ed).
UpToDate
, Waltham, MA: UpToDate, Inc.; 2009.
Khan F, Sachs H, Pechet L, et al.
Guide to Diagnostic Testing
. Philadelphia, PA: Lippincott Williams & Wilkins; 2002.
OSTEOPOROSIS
Definition
The World Health Organization defines osteoporosis as bone mineral density (BMD) more than 2.5 standard deviations below the mean of young normal controls (T-score).