Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (624 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md


Sepsis
: Unexplained respiratory alkalosis may be the earliest sign of sepsis. It may progress to cause metabolic acidosis, and the mixed picture may produce a normal pH; low HCO
3
−
is useful for recognizing this. With deterioration and worsening of metabolic acidosis, the pH falls.
Salicylate poisoning
characteristically shows poor correlation between serum salicylate level and presence or degree of acidemia (because as pH drops from 7.4 to 7.2, the proportion of nonionized to ionized salicylate doubles and the nonionized form leaves the serum and is sequestered in the brain and other organs, where it interferes with function at a cellular level without changing blood levels of glucose, and so on). Salicylate poisoning in adults typically causes respiratory alkalosis, but in children, this progresses rapidly to mixed respiratory alkalosis/metabolic acidosis and then to metabolic acidosis (in adults, metabolic acidosis is said to be rare and a near-terminal event).
Isopropyl
(rubbing) alcohol poisoning produces enough circulating acetone to produce a positive nitroprusside test (it, therefore, may be mistaken for DKA; consequently, insulin should not be given until the blood glucose is known). In the absence of a history, positive serum ketone test associated with normal AG, normal serum HCO
3
−
, and normal blood glucose suggests rubbing alcohol intoxication.
A change in chloride concentration independent of
, or out of proportion to, changes in sodium usually indicates an acid–base disorder.
*
Written by Michael Snyder, MD and Mary Williamson, PhD.
*
Written by Mary Williamson, PhD.
Chapter
14
Toxicology and Therapeutic Drug Monitoring
Amanda J. Jenkins
T
oxicology is the study of the adverse effects of chemicals on living organisms. Clinical toxicology is a subspecialty with emphasis on management of a poisoned patient. The application is focused on human beings but may be equally applied in veterinary medicine. The principles of clinical toxicology are applied to two main areas—emergency toxicology and therapeutic drug monitoring. Emerging fields include addiction medicine and pain management.

EMERGENCY TOXICOLOGY
Purpose
The majority of poisoned patients enter the health care system in the emergency department. Treatment is often based on exposure history and signs and symptoms of poisoning based on physical examination. Laboratory testing may be performed to confirm the physician’s diagnosis or to identify a toxin in the absence of a differential diagnosis.
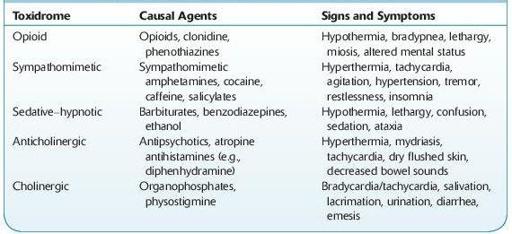
Knowledge of toxidromes is important as a starting point for patient evaluation (Table
14-1
). These consist of a collection of signs and symptoms that are typically produced by specific toxins.
TABLE 14–1. Signs and Symptoms of Common Toxidromes
Testing offered by clinical toxicology laboratories consists of screening and confirmation.
Screening tests are usually conducted on urine. These require little or no sample preparation and are frequently immunoassay based. These tests have high sensitivity; however, they have limitations due to moderate specificity. Many commercially available tests cross-react with multiple drugs within a class due to choice of target drug. They may also be sensitive to adulterants. Clinicians must be aware of the commercial tests utilized in their laboratory, as cross-reactivities differ between manufacturers and within manufacturers over time.
These tests are typically performed on automated chemistry analyzers. Although individual drug–drug classes are available, many hospital laboratories offer these tests as panels and are available as “stat” tests.
Immunoassay testing may be based on