Secondary Schizophrenia (146 page)
Read Secondary Schizophrenia Online
Authors: Perminder S. Sachdev

man . . . full of health . . . of intact memory . . . does not at
simple and complex visual hallucinations
all take these visions for reality”
[1].
Bonnet stressed
(VHs) in the absence of a psychiatric
the mental normality of his grandfather.
disorder.
Although there were many reports of visual hallu-
r
Most cases are due to damage to some part of
cinations in the nineteenth century, most of these were
the visual system.
due to lesions of the brain and were often associated
r
A deafferentation hypersensitivity model best
with other signs such as epilepsy and stroke
[2].
In the
explains the syndrome.
twentieth century, interest in this phenomenon slowly
r
increased. The eponym “Charles Bonnet Syndrome”
There are reasons to believe that complex
was introduced in 1996 by de Morsier in recognition
hallucinations are generated in a part of the
of the contribution of his fellow Genovese
[3].
In 1967,
cerebral cortex extending from superior
de Morsier
[4]
summarized the main papers up to that
temporal cortex ventrally to the
time (18 cases), but even as late as 1989, only about
parahippocampal gyrus.
r
46 cases had been reported
[5].
Since then, there has
The hallucinations are usually pleasant
been an escalation of interest, research, and publica-or neutral and eventually disappear, although
tions on the topic. In recent years, there have been sev-complex hallucinations may last several years.
r
eral reviews of the literature
[6, 7, 8, 9].
In some cases, the hallucinations seem to be
the first signs of dementia.
Definition
The simplest definition of Charles Bonnet Syndrome
(CBS) is that it consists of VHs in a patient who
The syndrome takes its name from Charles Bon-
is psychologically normal and has full cognition and
net, a biologist and philosopher of science, who in
insight, that is, realizes that the hallucinations are
1770 described the hallucinations experienced by his
not real, even if initially he is fearful that he might
grandfather Charles Lullin
[1]
. Lullin had cataracts
be “going mad.” These cases can be subdivided into
removed from both eyes and, although the opera-
three groups. The largest group (group A) consists of
tions were at first successful, eventually at the age
cases in which there is visual impairment and appar-
of 89 years he became completely blind in one eye
ently no other contributory factor. In the second group
and had very little sight in the other. He then devel-
(group B), there is visual impairment but the occur-
oped visual hallucinations (VHs). As described by
rence of VHs is dependent on another factor or “trig-Bonnet, Lullin saw before him “figures of men and
ger.” In the third group (group C), there is no visual
women, birds, carriages, battlements . . . He saw these
impairment but VHs are triggered in a variety of ways.
369
figures make different movements, approach, move
There are many other classifications
[4, 8, 10].
Related Concepts – Section 4
Visual impairment includes any injury from retina
[35],
HIV
[36],
predementia Alzheimer’s
[6],
Parkin-to extrastriate cortex but also includes light restriction
sons’s
[37, 38,
39],
and pineal tumor
[40].
Whole brain
as in corneal scarring or cataract. The commonest con-radiation therapy following removal of a metastatic
ditions are age-related macular degeneration (AMD),
adenocarcinoma near the right cuneus caused the
glaucoma, and cataract
[8, 11].
Other conditions are
emergence of hallucinations consisting of memories
optic neuritis
[12],
enucleation of the eye
[13],
retini-of distinct people and events
[41].
These were unlike
tis pigmentosa
[14],
diabetic retinopathy
[11],
corneal
the typical CBS hallucinations and more like the expe-disease
[11],
destruction of optic nerves by tumor
[15],
riential recollections described by Penfield and Perot
macular photocoagulation
[16],
macular translocation
[42].
Perceptual isolation can lead to VHs
[43, 44,
[17]
, and occipital lobe damage
[18, 19].
45].
Isolation and life-threatening stress (e.g., among
Three other types of visual “hallucinations” may be
hostages) can also cause hallucinations
[46].
De Mor-included in group A. Photopsias are flashes of light
sier
[4]
thought that CBS was a disease of old age. How-or the appearance of small simple discs of light, usu-ever, there are now several well-attested cases of CBS in
ally white but sometimes colored, generally ascribed
children
[47, 48, 49].
Nevertheless, because visual disto some irritation in the retina. Palinopsia refers to
ease is commoner in old people, likewise, CBS is more
the abnormal persistence of a visual image. This is
evident.
not an after-image, however, because there is no rever-Some investigators would restrict CBS to groups A
sal of luminance or color. Although palinopsia occurs
and B
[8].
This is a matter of choice. The existence of
in patients with visual impairment, it has also been
group C is not in doubt. The clearest example of this
reported in people with normal vision
[20].
Visual
is the occurrence of VHs in normal people who have
“auras” occur in association with migraine but can
been blindfolded for a day or more
[50, 51,
52].
also occur independently
[21, 22, 23].
The commonest
Attempts have been made to exclude visual defects
type is referred to as “fortifications” because of a fan-as a critical factor
[4, 6].
For example, some CBS
cied resemblance to castles. The multicolored zigzags
patients have normal visual acuity, such as in some
spread from the point of gaze out to the periphery
cases of cerebral infarct
[53]
and cases of glaucoma.
of the visual field in 20 to 30 minutes. It is believed
This argument is faulty because acuity is not an ade-to be due to a form of “spreading depression,” partly
quate measure of visual impairment
[54].
The lists of
because there is total blindness in the wake of the
conditions given here for groups A, B, and C are not
zigzags
[22]
. Photopsias, palinopsia, and auras are not
exhaustive.
usually included in the CBS category.
Trigger factors capable of generating VHs in
patients with visual impairment include: tramadol (an
Simple and complex hallucinations
opioid) in a patient with diabetic retinopathy
[24],
opi-Most writers
[6, 8,
55]
specify that the VHs be “com-oids (morphine) in a patient with retinitis pigmen-plex” to be regarded as CBS. By this is meant that the
tosa
[25],
laser iridotomy in a patient with glaucoma
patient sees elaborate visions of people, animals, var-
[26],
brimonidine in eye drops used for glaucoma
[27],
ious identifiable objects, scenery, buildings, text, and
social isolation
[28]
, and strong emotional states, for
so on. It is now clear that simpler visions also occur,
example, bereavement
[29].
such as rotating discs of light and simple auras, leaves,
Finally, group C consists of cases without visual
branching structures, geometrical arrangements, such
impairment but in which VHs occur. Of course, there
as chess boards, netting, egg crates, and tessellations –
are many drugs (hallucinogens) whose main effect
often depicted as lines crisscrossing at right angles
is to cause hallucinations
[30].
In addition, several
(Figure 30.1).
Sometimes the elements separate into
other drugs, not regarded as hallucinogens, may cause
lozenges or tiles. These simpler hallucinations are less
VHs in certain circumstances. Very often, they are
obvious to the patient and may not be very different
medicaments being given for another condition, for
to after-images. Because they are less dramatic than
example, drugs acting on the GABAergic system of
the complex hallucinations, do not move, may be small
the brain such as digoxin
[31,
32],
estrogen
[33],
or
or faint, and may be short lasting, they are not always
drugs used to treat Parkinson’s, such as amantadine
reported by the patient. Nevertheless, many patients
[34]
or amitriptyline
[28].
Certain nonvisual diseases
experience both simple and complex VHs and it is
370
are capable of inducing VHs, for example, migraine
possible that they have a common origin. The patient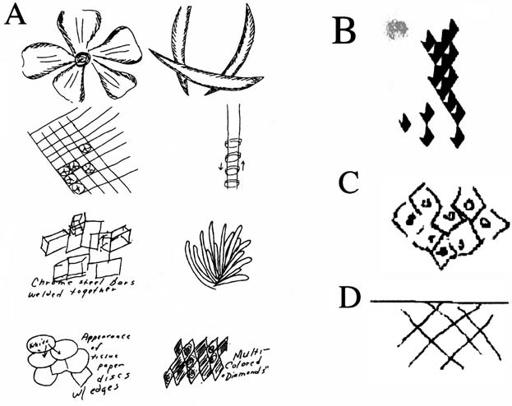
Chapter 30 – The Charles Bonnet Syndrome
Figure 30.1
Examples of simple
hallucinations. A. Sketches by patient with
occipital lobe damage (from
[19]).
B. Sketch by patient with right occipital
infarct; rhomboids are about 0.5
◦
in size
and appear in the left visual field (from
[56]).
C. Hallucinations from two patients
with eye disease (from
[57]).
should be carefully questioned and shown some exam-
areas where spontaneous activity was high. The con-
ples of these “simple” hallucinations.
clusion may therefore be reached that these geometric
An important feature of central visual pathways is
hallucinations are due to increased activity in V1 and
that the lower-order cortical areas, especially V1 to V5,
V2, even if the perceptive process occurs at a higher
are strictly visuotopic (retinotopic). This is true but to
level.
a much coarser degree for the higher-order areas
[58,
An extension of this line of thought is that the
59]
, where cells become specialized for the detection of
observed hallucination will be determined by the
complex features, such as faces, buildings, tools, text,
highest level in the visual pathway at which there is
and scenery. The cells in these areas may not be insen-
“marked” spontaneous activity. In some way, the brain
sitive to simpler stimuli, but they are much more sen-must distinguish this “marked” activity from ordi-
sitive to particular objects. It is likely, therefore, that
nary ongoing spontaneous activity. It may be that the
the simpler geometric hallucinations have closer ties
“marking” is achieved by a “bursting” pattern, which
with the lower-order visual areas. This idea finds sup-is capable of reaching a threshold in the perceptual
port in my own observations
[60].
These were made
process that cannot be reached by the ordinary spon-
following the occurrence of a macular hole (foveal reti-taneous activity
[9].
Bursty firing is well known to
nal detachment) in each of my eyes at the same time.
exert powerful transmission effects
[61].
The elec-These hallucinations
(Figure 30.2)
were small and faint
troencephalogram during hallucinations in patients