Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (399 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
13.89Mb size Format: txt, pdf, ePub
Patients with a personal or family history of mucosal bleeding (except for VWD type 3, where the bleeding is severe, and type 2N that mimics hemophilia) (see below). Females with severe menorrhagia presenting at menarche. Although VWD is relatively common, not all patients are diagnosed because not all have a marked bleeding history.
Laboratory Findings
Because the clinical manifestations of VWD and platelet defects are similar, the laboratory workup for platelet function and for VWD should be initiated simultaneously, except for cases with a definite family history.
1. vWF Ag (vWF:Ag).
2. Factor VIII coagulant. 3. Ristocetin cofactor (vWF:RCo) assay measures vWF activity. A ratio vWF:RCo/vWF:Ag <0.7 is indicative of a qualitative vWF defect.
4. VWF activity: A new latex immunoassay for the quantitation of vWF has recently become commercially available (HemosIL
™
). It was demonstrated to have very high sensitivity and specificity for vWF activity.
5. The collagen-binding assay is another functional assay used by some laboratories.
1. VWF multimers is a useful assay to determine various subtypes of the disease. It should be ordered only when the vWD diagnosis has been established.
2. Ristocetin-induced platelet aggregation (RIPA). In this assay, the patient’s platelets and plasma are used as a source of vWF.
3. Genetic tests are now being developed.
Seven clinical variants
have been described based on laboratory results and clinical history:
1. VWD type 1 (70–80% of cases) is a quantitative defect with mild bleeding. The diagnosis can be challenging and might require repeated testing.
2. VWD type 2A (10–15% of cases) is a qualitative defect with moderate to severe bleeding. There is absence of high molecular weight VWF multimers.
3. VWD type 2B is a rare qualitative defect with a “gain-of-function” point mutation in the GP1b binding domain of VWF. Patients have spontaneous platelet agglutination resulting in thrombocytopenia. There is absence of high molecular weight VWF multimers. DDAVP administration is contraindicated.
4. VWD type 2M is a rare, mostly autosomal dominant, qualitative defect with moderate to severe bleeding. There is a defect in the GP1b binding domain of VWF, preventing binding to platelets. In types 2A, 2B, and 2 M, there is a low ratio (<0.7) of VWF activity to antigen.
5. VWD type 2N is a rare qualitative defect with moderate to severe bleeding. There is a defect in the FVIII binding domain of vWF. It simulates hemophilia.
6. VWD type 3 is a rare quantitative defect with severe bleeding. These patients may develop alloantibodies to VWF after receiving multiple transfusions.
7. Platelet-type VWD is not a genuine VWD variant (see p. 450), but a qualitative defect in platelets caused by a gain of function in the GP1b receptor on platelets. That leads to increased avidity for VWF resulting in spontaneous platelet agglutination and thrombocytopenia. Platelet-type VWD can be differentiated from VWD type 2B by mixing or cryoprecipitate studies. Platelets from Bernard-Soulier syndrome (see p. 450) do not aggregate in the presence of ristocetin. The condition must be differentiated from VWD.
9-5
.
TABLE 9–5. Subtypes of von Willebrand Disease
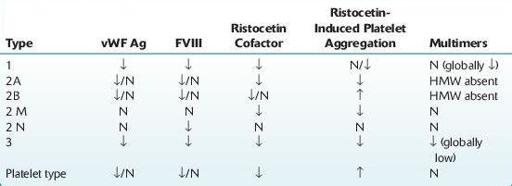
N, normal; ↓, decreased; ↑, increased with low-dose ristocetin; HMW, high molecular weight multimers.
Other books
Panther's Claim (Bitten Point #2) by Eve Langlais
Hannah's Gift by Maria Housden
Torment and Terror by Craig Halloran
Demon Night by Meljean Brook
The Crystal World by J. G. Ballard
Chase and Seduction by Randi Alexander
Taste of Darkness by Katie Reus
A Sweet Deal (Crimson Romance) by Tillery, Monica
Cordimancy by Hardman, Daniel