Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (522 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
12.87Mb size Format: txt, pdf, ePub
TABLE 12–1. Staging of Acute Kidney Injury
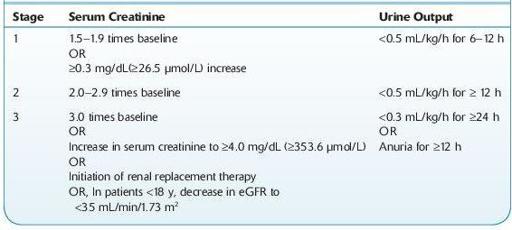
eGFR, estimated glomerular filtration rate.
Source: Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group.
KDIGO clinical practice guideline for acute kidney injury.
Kidney Int.
2012;2(Suppl):1–138.
Who Should Be Suspected?
Patients with AKI present in a variety of ways:
Patients with symptoms suggestive of uremia. The term uremia describes the clinical syndrome associated with retention of the end products of nitrogen metabolism due to severe reduction in renal function. It can be a consequence of either acute or chronic renal disease.
12-1
). Microscopic examination is normal in most cases of prerenal disease. The presence of RBC casts or dysmorphic RBCs indicates glomerular disease, whereas finding cellular debris or granular casts suggests ischemic or nephrotoxic AKI. Urine specific gravity is of limited value in establishing the etiology of AKI.
Other books
Women's Bodies, Women's Wisdom by Christiane Northrup
Bound to the Alpha: The Bundle by Viola Rivard
Bayou Trackdown by Jon Sharpe
Splitting Up and Park Hyatt Hotel by Galatée de Chaussy
Pure Lust Vol. 2 by Parker, M. S., Wild, Cassie
The Art of Keeping Secrets by Patti Callahan Henry
Total Rush by Deirdre Martin
Entangled With the Thief by Kate Rudolph
The Second-last Woman in England by Maggie Joel
Ascending by James Alan Gardner