Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (523 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

Patients with postrenal disease are diagnosed based on clinical presentation and imaging studies.
N
-acetyl-β-glucosaminidase (NAG), neutrophil gelatinase–associated lipocalin (NGAL), retinol-binding protein and interleukin (IL)-18.
12-2
.
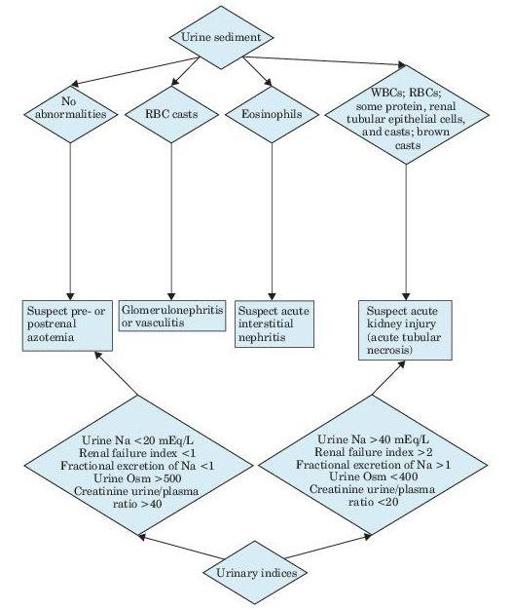
Figure 12–1
Algorithm for the diagnosis of acute kidney injury.
TABLE 12–2. Urinary Diagnostic Indices in Acute Kidney Injury
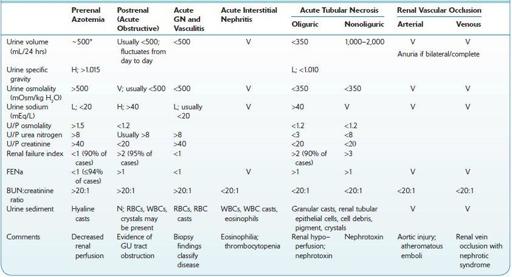
H, high; L, low; N, normal; U/P, urine/plasma ratio; V, variable.
*Polyuria may be present.
Sources: Andreoli TE, et al., eds.
Cecil Essentials of Medicine
, 2nd ed. Philadelphia, PA: WB Saunders; 1990;212; Okum DE. On the differential diagnosis of acute renal failure.
Am J Med
. 1981;71:916; Schrier RW. Acute renal failure: pathogenesis, diagnosis, and management.
Hosp Pract
. 1981;16:9398; Miller TR, et al. Urinary diagnostic indices in acute renal failure: a prospective study.
Ann Intern Med
. 1978;89:47.
Suggested Readings
Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO clinical practice guideline for acute kidney injury.
Kidney Int.
2012;(Suppl 2):1–138.
http://www.kdigo.org/clinical_practice_guidelines/pdf/KDIGO%20AKI%20Guideline.pdf
Vaidya VS, Ferguson MA, Bonventre JV. Biomarkers of acute kidney injury.
Annu Rev Pharmacol Toxicol.
2008;48:463–493.
ACUTE TUBULAR NECROSIS
Definition
Candidates for investigation include patients (in most cases hospitalized) with exposure to a nephrotoxin (e.g., therapy with aminoglycoside or amphotericin B, radiologic contrast materials, heavy metals, cisplatin, ethylene glycol, or heme pigments such as free hemoglobin or myoglobin), severe trauma, hemorrhage, hypotension, surgery or sepsis, and recent-onset oliguria or anuria.