Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (530 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
4.03Mb size Format: txt, pdf, ePub
The clinical spectrum of GN comprises:
Asymptomatic subnephrotic proteinuria without hematuria.
12-3
.
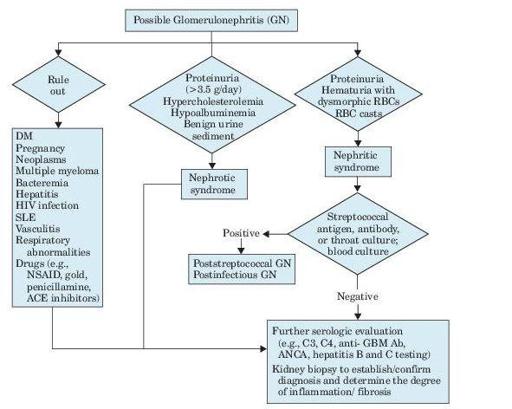
Figure 12–3
Algorithm for evaluation of glomerulonephritis.
Suggested Reading
Klinger M, Mazanowska O. Primary idiopathic glomerulonephritis: modern algorithm for diagnosis and treatment.
Pol Arch Med Wewn.
2008;118(10):567–571.
GLOMERULONEPHRITIS, MEMBRANOPROLIFERATIVE
Definition
Other books
Death at the Door by K. C. Greenlief
Storm Front (The Charistown Series) (Volume 2) by Lisa N. Paul
Dusk of Defiance (The Era of Ensemble Book 1) by Woosey, JP
Deborah Brown - Madison Westin 07 - Kidnapped in Paradise by Deborah Brown
The Witch House of Persimmon Point by Suzanne Palmieri
The Girl With Glass Feet by Ali Shaw
Unbroken by Jasmine Carolina
Double the Trouble by Tiffany Lordes
What falls away : a memoir by Farrow, Mia, 1945-