Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (616 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

BOOK: Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis
3.68Mb size Format: txt, pdf, ePub
Metabolic alkalosis patients may be volume depleted and chloride responsive or have volume expansion and be chloride resistant.
13-4
) are a graphic solution of the Henderson-Hasselbalch equation, which predicts the HCO
3
‒
value for each set of pH/ pCO
2
coordinates. They also allow a check of the consistency of ABG and automated analyzer determinations, since these may determine the total CO
2
content, of which 95% is HCO
3
−
.
2
coordinate is outside the 95% confidence band, then the patient has at least two acid–base disturbances.
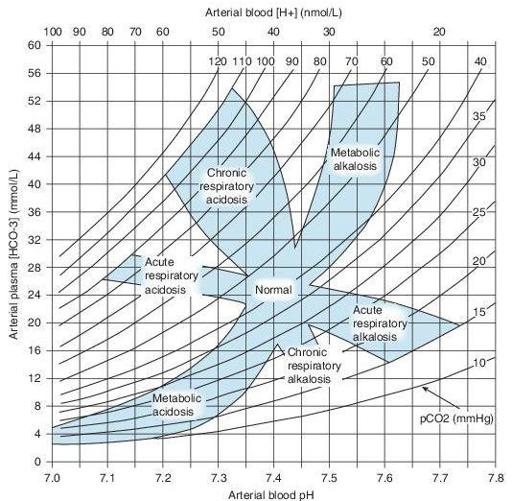
Figure 13–4
Acid–base map. The values demarcated for each disorder represent a 95% probability range for each pure disorder. Coordinates lying outside these zones suggest mixed acid–base disorders.
METABOLIC ACIDOSIS
With Increased Anion Gap (AG >15 mmol/L)
DM (AG frequently >25 mmol/L)
Other books
Earth Girls Aren't Easy by Charlene Teglia
The Dreamer's Curse (Book 2) by Honor Raconteur
The Kiss of Deception by Mary E. Pearson
i 8383b91bded90ce1 by Unknown
Lying by Lauren Slater
Penny Dreadful Multipack Vol. 1 (Illustrated. Annotated. 'Wagner The Wehr-Wolf,' 'Varney The Vampire,' 'The Mysteries of London Vol. 1' + Bonus Features) (Penny Dreadful Multipacks) by George W. M. Reynolds, James Malcolm Rymer
Dark Swan Bundle by Richelle Mead
Something About Love: A YA contemporary romance in verse by Johnson, Elana
The Bomber by Liza Marklund
Plains Song by Wright Morris