Secondary Schizophrenia (24 page)
Read Secondary Schizophrenia Online
Authors: Perminder S. Sachdev

the ear. Schizophr Res, 1995.
17
:
A.,
et al.
State dependent changes
Br J Psychiatry, 1991.
158
:328–
289–91.
in error monitoring in
36.
88. Bartlett M. The sensory acuity of
schizophrenia. J Psychiatr Res,
78. Karp B. I., Garvey M., Jacobsen L.
psychopathic individuals: a
2004.
38
:347–56.
K.,
et al.
Abnormal neurologic
comparison of the auditory acuity
69. Kathmann N., Von Recum S.,
maturation in adolescents with
of psychoneurotic and dementia
Haag C.,
et al.
Electrophysio-
early-onset schizophrenia. Am J
praecox cases with that of normal
logical evidence for reduced latent
Psychiatry, 2001.
158
:118–22.
individuals. Psychiatr Q, 1935.
inhibition in schizophrenic
79. Hyde T., Hotson J., Kleinman J.
9
:422–5.
patients. Schizophr Res, 2000.
Differential diagnosis of
89. Ludwig A. M., Wood B. S., Jr.,
58
45
:103–14.
choreiform tardive dyskinesia.
Downs M. P. Auditory studies in
Chapter 4 – The neurologic examination in schizophrenia
schizophrenia. Am J Psychiatry,
examination. Psychiatr J Univ Ott,
106. Rubino F. A. Neurologic
1962.
119
:122–7.
1989.
14
:554–6.
complications of alcoholism.
90. Hawkes C. Olfaction in
98. Sanders R. D., Joo Y. H., Almasy
Psychiatr Clin North Am, 1992.
neurodegenerative disorder. Adv
L.,
et al.
Are neurologic
15
:359–72.
Otorhinolaryngol, 2006.
63
:
examination abnormalities
107. Casanova M. F. Wernicke’s disease
133–5.
heritable? A preliminary study.
and schizophrenia: a case report
91. Kopala L., Clark C., Hurwitz T.
Schizophr Res, 2006.
86
:172–80.
and review of the literature. Int J
Olfactory deficits in neuroleptic
99. Jenkyn L. R., Walsh D. B., Culver
Psychiatry Med, 1996.
26
:319–28.
naive patients with schizophrenia.
C. M.,
et al.
Clinical signs in
108. Allen D. N., Goldstein G., Forman
Schizophr Res, 1992.
8
:245–
diffuse cerebral dysfunction.
S. D.,
et al.
Neurologic
50.
J Neurol Neurosurg Psychiatry,
examination abnormalities in
92. Sirota P., Davidson B., Mosheva
1977.
40
:956–66.
schizophrenia with and without a
T.,
et al.
Increased olfactory
100. Arango C., Bartko J. J., Gold J. M.,
history of alcoholism.
sensitivity in first episode
et al.
Prediction of
Neuropsychiatry Neuropsychol
psychosis and the effect of
neuropsychological performance
Behav Neurol, 2000.
13
:184–7.
neuroleptic treatment on olfactory
by neurological signs in
109. Goldstein G., Allen D. N., Sanders
sensitivity in schizophrenia.
schizophrenia. Am J Psychiatry,
R. D. Sensory-perceptual
Psychiatry Res, 1999.
86
:
1999.
156
:1349–57.
dysfunction in patients with
143–53.
101. Sanders R., Shuepbach D.,
schizophrenia and comorbid
93. Collins L., Stone L. Pain
Keshavan M. S.,
et al.
Neurologic
alcoholism. J Clin Exp
sensitivity, age and activity level in
exam abnormalities and
Neuropsychol, 2002.
24
:1010–16.
chronic schizophrenics and
neuropsychological performances
110. Kinney D. K., Yurgelun-Todd D.
normals. Br J Psychiatry, 1966.
in neuroleptic-naive psychosis.
A., Woods B. T. Neurologic signs
112
:33–5.
J Neuropsychiatr Clin Neurosci,
of cerebellar and cortical sensory
94. Nasrallah H. A., Tippin J.,
2004.
16
:480–7.
dysfunction in schizophrenics and
Mccalley-Whitters M.,
et al.
102. Moles J. K., Franchina J. J., Sforza
their relatives. Schizophr Res,
Neurological differences between
P. P. Neurological deficits and CT
1999.
35
:99–104.
paranoid and nonparanoid
findings in psychiatric patients.
111. Desmukh A., Rosenbloom M.,
schizophrenia: Part III.
Psychosomatics, 1998.
39
:394–5.
Pfefferbaum A.,
et al.
Clinical
Neurological soft signs. J Clin
103. Bae C. J., Pincus J. H. Neurologic
signs of cerebellar dysfunction in
Psychiatry, 1982.
43
:310–2.
signs predict periventricular white
schizophrenia, alcoholism and
95. Detre T., Bunney W. E. Jr. Human
matter lesions on MRI. Can J
their comorbidity. Schizophr Res,
vibration perception. II. A
Neurol Sci, 2004.
31
:242–7.
2002.
57
:281–91.
preliminary report on vibration
104. Murphy K. C. (2002)
112. Bartzokis G., Beckson M.,
perception in psychiatric patients.
Schizophrenia and
Wirshing D. A.,
et al.
Arch Gen Psychiatry, 1961.
velo-cardio-facial syndrome.
Choreoathetoid movements in
4
:615–8.
Lancet, 2002.
359
:426–30.
cocaine dependence. Biol
96. Fink M., Green M., Bender M. B.
105. Baumann N., Turpin J. C., Lefevre
Psychiatry, 1999.
45
:1630–5.
The face–hand test as a diagnostic
M.,
et al.
Motor and psycho-
113. Bauer L. O. Resting hand tremor
sign of organic mental syndrome.
cognitive clinical types in adult
in abstinent cocaine-dependent,
Neurology, 1952.
2
:46–58.
metachromatic leukodystrophy:
alcohol-dependent, and
97. Patten S. B., Lamarre C. J. The
genotype/phenotype
polydrug-dependent patients.
face–hand test: a useful addition
relationships? J Physiol Paris,
Alcohol Clin Exp Res, 1996.
to the psychiatric physical
2002.
96
:301–6.
20
:1196–201.
59
Section 2
The neurology of schizophrenia
5 Functionalneuroimaginginschizophrenia
Serge A. Mitelman, Jane Zhang, and Monte S. Buchsbaum
Acknowledgments
: This work was supported by
circulation-borne products of the liver and pancreas
NIMH grants P50 MH 66392–01, MH 60023, and
have made blood chemistry sampling and postmortem
MH 56489 to Dr. Buchsbaum and by NARSAD
assessment fruitful approaches, the regional com-Young Investigator and NIMH MH 077146 awards to
plexity and behavioral productions of the brain have
Dr. Mitelman.
made these methods less informative for the brain,
the target organ of schizophrenia. In this review, we
Facts box
describe brain–function research in psychiatry from
its inception with the electroencephalogram (EEG)
1. Functional imaging has shown decreases in
to the current advances in regional metabolism,
resting activity and the amount of activation
blood flow, receptor chemistry, and most recently,
by cognitive tasks in the frontal lobe,
the deficiencies in the dynamic connectivity of
temporal lobe, cingulate gyrus, and thalamus
circuits.
in schizophrenia.
2. Decreases in activity appear in regions that
Electroencephalography, cerebral
also show decreases in volume when
anatomical imaging techniques are used.
blood flow, and the earliest functional
3. The underlying etiology and pathogenesis of
imaging of schizophrenia
these activities and volume changes remain
Among the earliest observations in Jena, Germany, of
unclear.
Hans Berger, the developer of the electroencephalo-4. Psychotic symptoms include auditory and
gram, was the observation of diminished occipital
visual hallucinations, paranoid delusions or
alpha activity in patients with schizophrenia
[1].
This
paranoid trends, ideas of reference, ideas of
reduction in smooth rhythmic resting activity over
influence, catatonia, and atypical features
the visual cortex, which is observed in normal indi-such as complex perceptual distortions.
viduals when they open their eyes, is consistent with
Although a link between psychotic
modern computer analysis of the electrical signals
symptoms and basal ganglia, temporal lobe,
and with concepts of heightened sensory responsive-and frontal lobe pathology is supported,
ness, the symptoms of hallucinations, and complex
symptoms appear to be variable after the
regional changes in brain function seen in schizophre-onset of neuronal damage, and remission has
nia. The earliest cerebral blood oxygen and glucose
also been reported.
studies by Joseph Wortis and colleagues
[2]
at Belle-5. Treatment is largely symptomatic but links
vue Hospital in New York assessed arteriovenous dif-between brain region change and symptom
ference and did not find patients with schizophre-change are being established.
nia to be different from controls. Seymour Kety and
colleagues, in 1948 at the University of Pennsylva-nia, studied cerebral blood flow (CBF) and simi-
Brain function and schizophrenia
larly did not find differences in total CBF, but sug-Instruments for observing and assessing organ
gested that regional blood flow abnormalities might
function have been technical eye-opening scientific
exist
[3].The
current regional approach to brain imag-advances in understanding of disease in the last 100
ing in schizophrenia began with the work of David
60
years. Although the uniform tissue composition and
Ingvar and coworkers in Lund, Sweden
[4]
who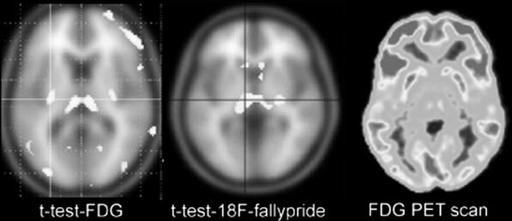
Chapter 5 – Functional neuroimaging in schizophrenia
Figure 5.1
Hypofrontality: individual
unmedicated patient with schizophrenia
showing areas in prefrontal cortex (including
Brodmann areas 10, 47, 9, 46) with relative
metabolic rate two standard deviations below
the normal control comparison group.
introduced regional functional imaging and staged
remains to be elucidated, for although hypofrontality
cognitive tasks to identify specific brain regions acti-has been demonstrated in neuroleptic-na¨ıve patients
vated by different mental activities and initiated the
[25],
treatment with antipsychotic agents may con-current direction of research in functional brain imag-tribute to its severity
[26].
ing in schizophrenia.
The newly emergent imaging technologies have