Wallach's Interpretation of Diagnostic Tests: Pathways to Arriving at a Clinical Diagnosis (220 page)
Authors: Mary A. Williamson Mt(ascp) Phd,L. Michael Snyder Md

Hirsutism may affect 5–10% of women of reproductive age. There are two conditions characterized by generalized hair growth that do not represent true hirsutism.
1. Hypertrichosis. It refers to excess terminal hair throughout the body. This is a rare condition that is usually caused by a drug, such as phenytoin, penicillamine, diazoxide, minoxidil, or cyclosporine. It can also occur in patients with systemic diseases, such as hypothyroidism, anorexia nervosa, malnutrition, porphyria, and dermatomyositis.
2. Increased vellus hair. It is the soft, unpigmented hair that covers the whole body, and it is androgen-independent hair.
Common Causes
Hirsutism is a result of the interaction between circulating serum androgens and the sensitivity of hair follicle to androgens. The most common causes of hirsutism are polycystic ovary syndrome and idiopathic hirsutism (Table
6-5
).
TABLE 6–5. Differential Diagnosis of Conditions Accompanied by Hirsutism and Their Specific Features
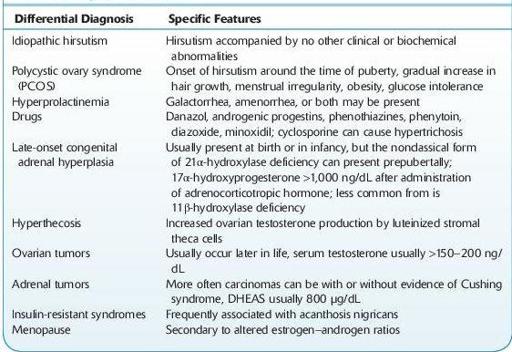
DHEAS, dehydroepiandrosterone sulfate.
The clinical approach to a patient with hirsutism includes the degree of androgen excess and its cause. The goal is to identify the small number of women who have potentially serious disorders such as androgen-secreting tumors or women with polycystic ovary syndrome.
I. History:
A. Menstrual history. Women with consistently regular menstrual cycles and symptoms of ovulation are unlikely to have severe hyperandrogenemia.
B. Time course of symptoms. Hirsutism occurring at a later age, with rapid onset, associated with the abrupt cessation of menses, or the presence of other features of virilization, is more often associated with potentially serious disorders, such as adrenal or ovarian tumors.
C. Weight history
D. Medication history
E. Family history
F. The presence of hirsutism alone is usually a benign condition.
II. Physical examination:
A. Look for and quantify increased hair in androgen-dependent regions.
B. Look for evidence of virilization, such as clitoral enlargement, deepening of voice, frontal balding, increased musculature, and loss of female body contour.
C. Look for evidence of Cushing syndrome, such as skin striae, thin skin, or bruising.
D. Body habitus. Height, weight, and a calculation of body mass index (BMI) should be obtained. Many women with polycystic ovary syndrome are obese.
E. Galactorrhea. The presence of any breast discharge is suggestive of hyperprolactinemia, and a serum prolactin level should be measured.
F. Abdominal and pelvic examinations. These examinations may reveal mass lesions producing androgen.
6-10
)
1. Serum androgens. Almost all women with hirsutism have an increased production rate of androgens, usually testosterone. Total serum testosterone is adequate to exclude testosterone-secreting tumors, but free testosterone may be necessary to identify smaller increases in testosterone, especially since the carrier protein for testosterone, sex hormone–binding globulin, is suppressed by hyperandrogenism and hyperinsulinemia (in patients with polycystic ovary disease). Free testosterone may be elevated, even with a normal total testosterone due to deceased serum binding. Serum DHEAS should be obtained if there is a suspicion of an adrenal androgen-secreting tumor.
2. Serum prolactin. If the patient also has irregular menses, serum prolactin should be measured for evaluation of possibility of hyperprolactinemia.
3. Serum LH. Women with polycystic ovary syndrome tend to have elevated serum LH concentrations and normal or low serum FSH concentrations.
4. 17α-hydroprogesterone (17α-OHP). Testing for nonclassic 21-hydroxylase deficiency should be considered in women with an early onset of hirsutism, hyperkalemia, or a family history of congenital adrenal hyperplasia. Basal serum 17α-hydroprogesterone concentrations may be only slightly high, especially late in the day. 17α-hydroprogesterone varies with menstrual cycle and increases with ovulation. A morning value of >300 ng/mL in the early follicular phase strongly suggests the diagnosis of 21-hydroxylase deficiency, which may be confirmed by an ACTH stimulation test. The response to ACTH is usually exaggerated.
5. Dexamethasone suppression testing. Circulating testosterone is derived from both ovarian and adrenal sources and precursors (androstenedione, DHEA, DHEAS). The administration of dexamethasone will suppress the production of adrenal androgens to a greater extent than it will suppress the production of ovarian androgens. Normal adrenal suppression indicates adrenal production of androgens such as congenital adrenal hyperplasia. Failure of suppression of DHEAS level strongly suggests the presence of an androgen-secreting adrenal tumor.
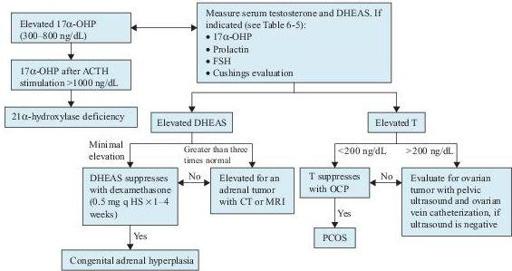
Figure 6–10
Diagnostic algorithm for hirsutism. 17
α
-OHP, 17
α
-hydroxyprogesterone; ACTH, adrenocorticotropic hormone; CT, computer tomography; DHEAS, dehydroepiandrosterone sulfate; FSH, follicle-stimulating hormone; MRI, magnetic resonance imaging; OCP, oral contraceptive pill; PCOS, polycystic ovary syndrome; T, testosterone.
6-10
)
An adrenal CT scan is recommended to look for an adrenal androgen-secreting tumor when serum DHEAS is markedly elevated. Pelvic ultrasonography with a transvaginal probe is an effective way to look for polycystic ovary or ovarian androgen-secreting tumors.
Suggested Readings
Barbieri RL, Ehrmann DA. Evaluation of women with hirsutism. In: Rose B, (ed).
UpToDate
, Waltham, MA: UpToDate, Inc.; 2009.
Barbieri RL, Ehrmann DA. Pathogenesis and cause of hirsutism. In: Rose B, (ed).
UpToDate
, Waltham, MA: UpToDate, Inc.; 2009.
Khan F, Sachs H, Pechet L, et al.
Guide to Diagnostic Testing
. Philadelphia, PA: Lippincott Williams & Wilkins; 2002.
GALACTORRHEA